Successful Right Subclavian Impella Placement in a Patient with Coarctation of the Aorta and Small Femoral Arteries: A Novel Access Approach for Mechanical Circulatory Support
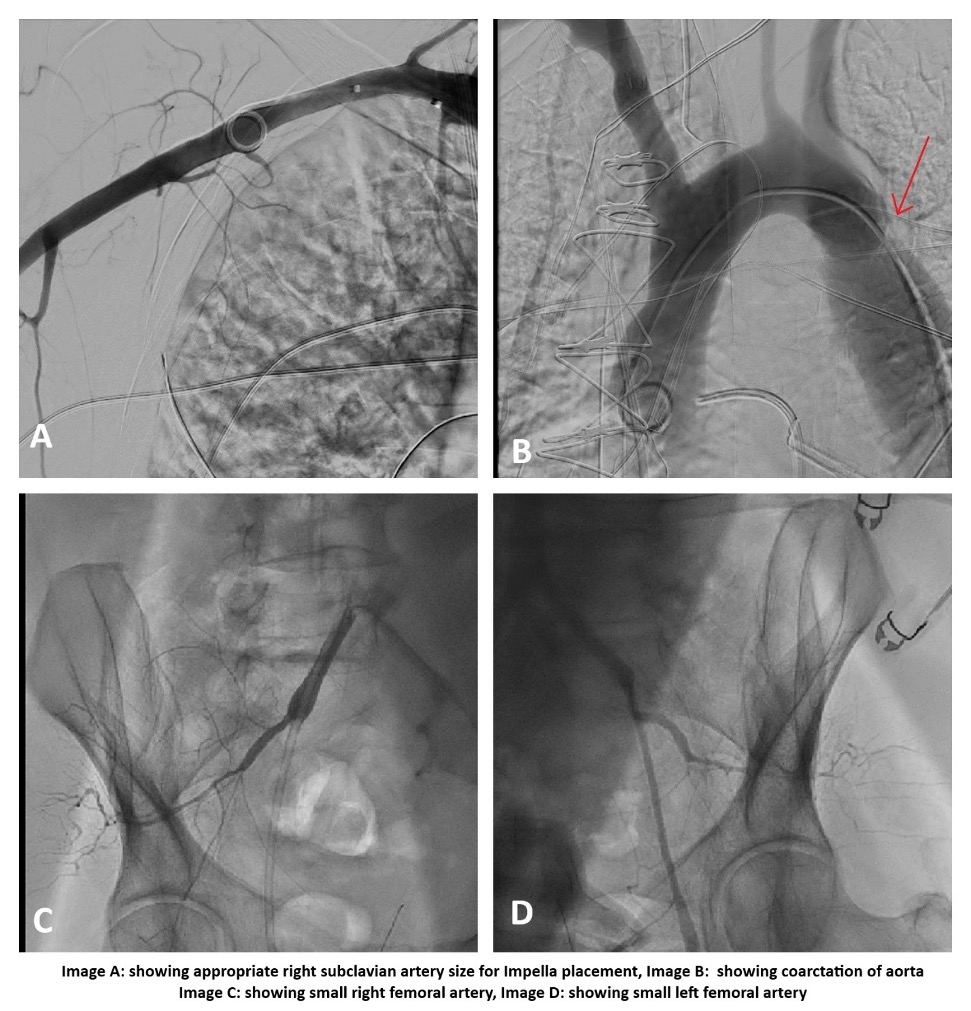
Abstract Body (Do not enter title and authors here): Case Description A 64-year-old male with a complex medical history, including mitral valve regurgitation/stenosis, severe aortic stenosis, mild coronary artery disease (CAD), coarctation of the aorta (diagnosed via pre-operative CT), pulmonary hypertension, patent foramen ovale (PFO), and chronic obstructive pulmonary disease (COPD), was admitted for elective surgical aortic valve replacement, mitral valve repair, and PFO closure. During surgery, the patient developed vasogenic shock requiring multiple vasopressors and inotropes. Despite placement of an intra-aortic balloon pump (IABP), the patient's condition continued to deteriorate, and he was transferred to the cardiac catheterization lab for coronary angiography and Impella support. The left femoral artery was accessed under ultrasound and fluoroscopy, but angiography revealed inadequate vessel caliber for a 14 Fr sheath. The right iliac artery was also too small. Due to aortic coarctation just distal to the left subclavian artery, this access site was excluded. Angiography of the right subclavian artery revealed suitable anatomy, so a pigtail catheter was advanced into the right subclavian artery. A 6 Fr sheath was inserted, and two pre-close sutures were deployed. An Amplatz Super Stiff wire was advanced in the ascending aorta, followed by successful insertion of a 14 Fr Impella sheath. A pigtail catheter was advanced into the LV apex, over which the 0.018-inch Impella wire was placed. The Impella CP device was then positioned, achieving flow of 3.5–3.8 L/min. The IABP and femoral sheath were removed. Coronary angiogram revealed only mild, non-obstructive CAD. The patient was transferred to the cardiac ICU in stable condition.
Discussion The Impella device is typically placed via transfemoral access. In patients with small-caliber femoral arteries or complex aortic anatomy, alternative routes must be considered. In this patient, coarctation of the aorta distal to the left subclavian artery and inadequate femoral access precluded traditional insertion sites. Right subclavian access was successfully used for Impella CP placement, with favorable hemodynamic support and outcome. To our knowledge, this is the first reported case of right subclavian Impella placement in a patient with both aortic coarctation and small femoral arteries. This case highlights the feasibility and safety of using the right subclavian artery as an alternative access route in selected patients with complex vascular anatomy.
Reaz, Shams
(
Mclaren - Flint
, Flint , Michigan , United States )
Almorsy, Khaled
(
Mclaren - Flint
, Flint , Michigan , United States )
Pitasari, Josephine
(
Mclaren - Flint
, Flint , Michigan , United States )
Munir, Ahmad
(
Mclaren - Flint
, Flint , Michigan , United States )
Author Disclosures:
Shams Reaz:No Answer
| Khaled Almorsy:DO NOT have relevant financial relationships
| Josephine Pitasari:DO NOT have relevant financial relationships
| Ahmad Munir:No Answer