Pembrolizumab-Induced Myositis Unmasking Double M Syndrome with Smoldering Myocarditis
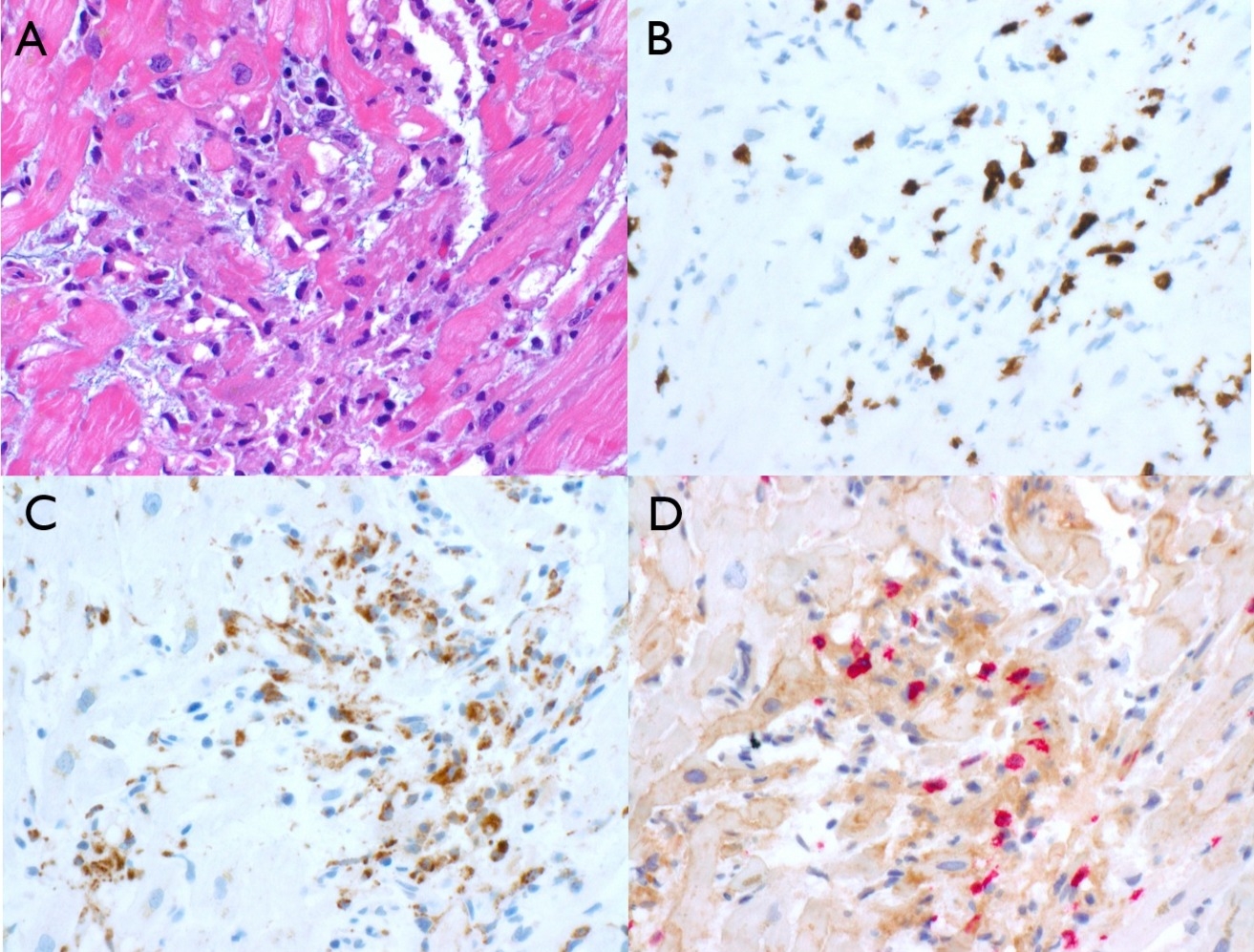
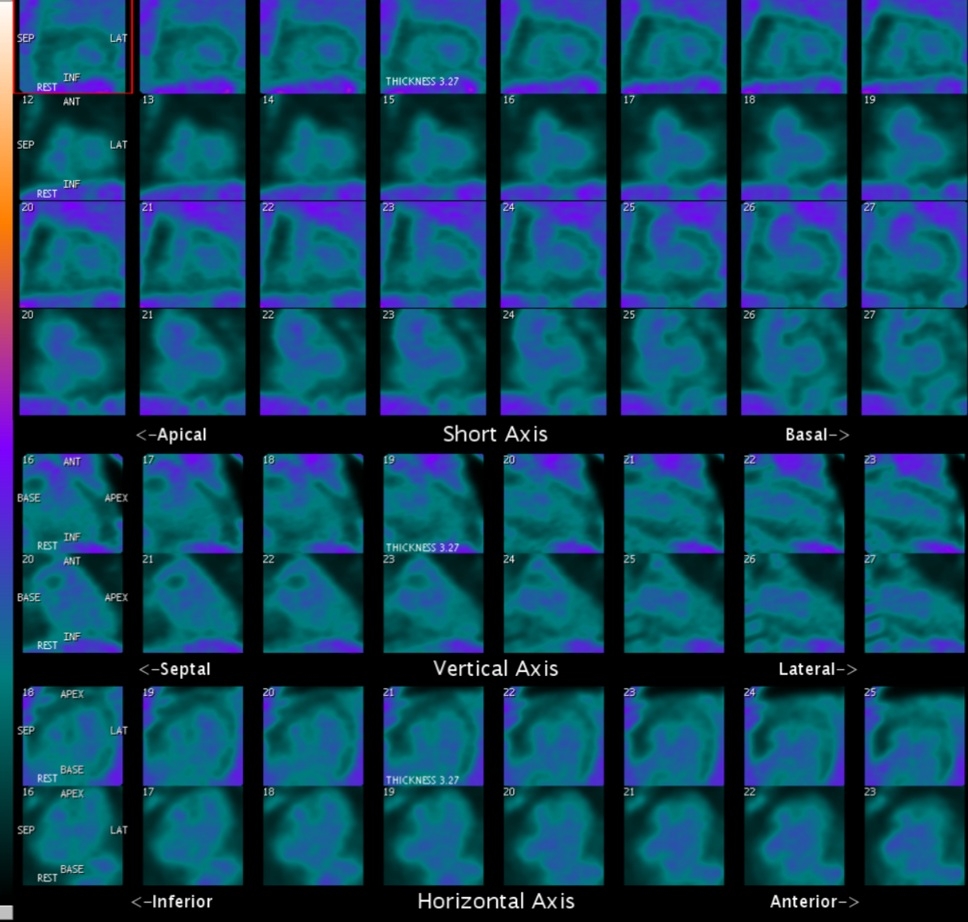
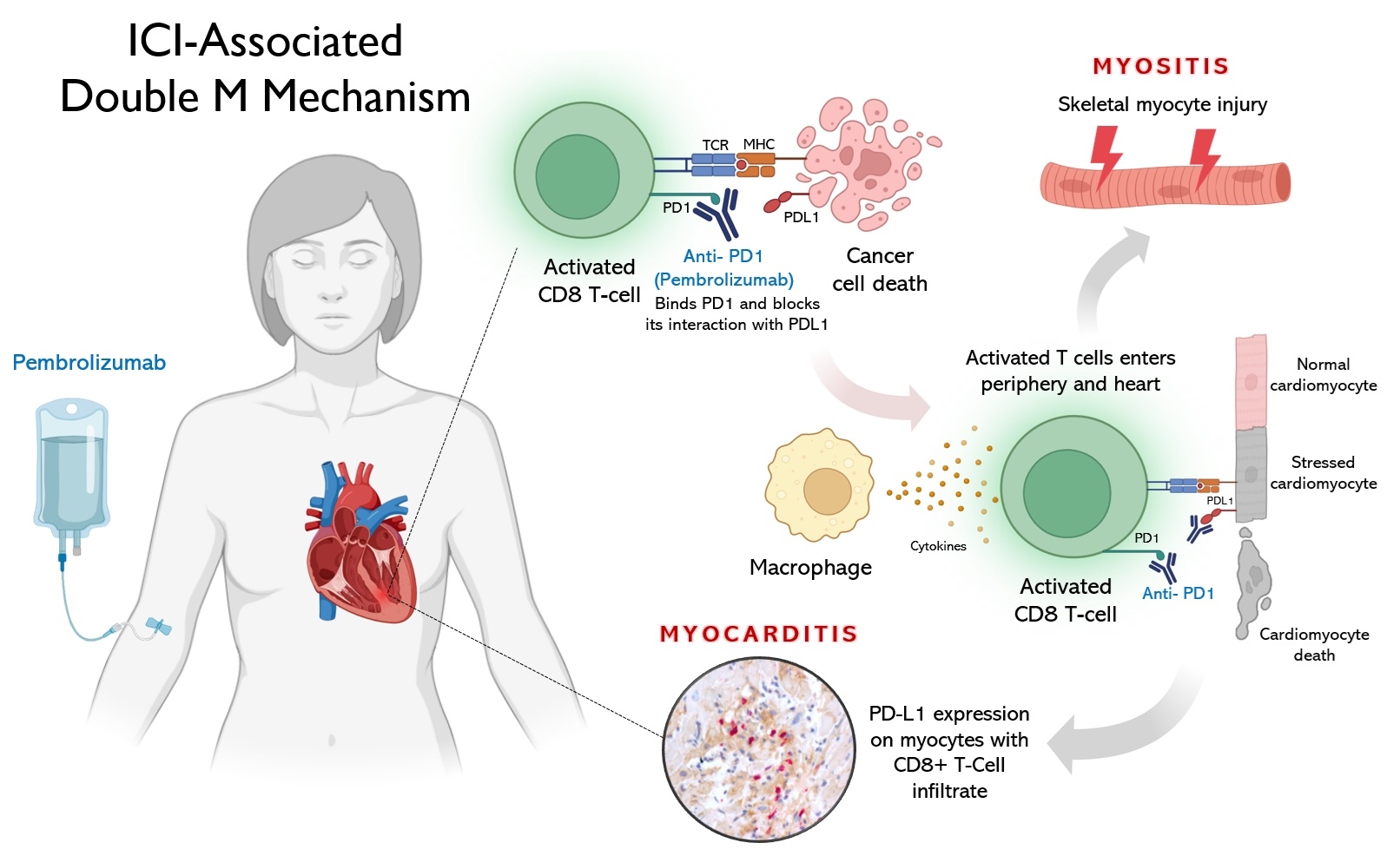
Abstract Body (Do not enter title and authors here): Background Immune checkpoint inhibitors (ICIs), such as pembrolizumab, have revolutionized cancer therapy but can trigger immune-related adverse events (irAEs), including myocarditis and myositis. Double M syndrome, myositis with concurrent myocarditis, is a rare, high-risk phenotype typically presenting acutely, though smoldering presentations are often underrecognized and constitute a diagnostic challenge. Clinical case A 67-year-old woman with stage IIb triple-negative breast cancer, treated with pembrolizumab-carboplatin/paclitaxel followed by doxorubicin/cyclophosphamide per KEYNOTE-522 protocol, presented four months after completing ICI therapy with worsening myalgias, weakness, low-grade fever, and transaminitis. Labs revealed elevated CK (7,760 U/L), transaminases (AST 369 U/L, ALT 626 U/L). ECG showed sinus tachycardia and diffuse ST depressions, with troponin-I (>15,000 ng/L), and CK-MB (185 ng/mL). TTE demonstrated preserved LVEF without wall motion abnormalities. Differential diagnoses included non-ST elevation myocardial infarction, ICI-related myocarditis, and viral myocarditis. Decision-Making Initial ACS management was initiated but discontinued after coronary angiography showed non-obstructive disease. Endomyocardial biopsy (EMB) revealed lymphocyte-predominant myocarditis with CD8+ cytotoxic T-cell infiltrates and PD-L1 overexpression in myocytes, confirming ICI-associated myocarditis (Figure 1). She was treated with pulse-dose methylprednisolone (1 g/day x 5 days), followed by oral prednisone taper. Follow-up cardiac PET/CT at two months showed complete resolution of myocardial inflammation (Figure 2). Conclusion This unique case illustrates a rare, delayed-onset presentation of pembrolizumab-induced Double M syndrome with smoldering myocarditis (Figure 3) and myositis, highlighting the importance of considering ICI-related myocarditis even in asymptomatic or subacute settings post-immunotherapy to avoid fatal cardiac complications. EMB played a critical role in diagnosis and tailored corticosteroid therapy. Timely recognition and coordinated multidisciplinary management are crucial for improving outcomes in ICI-related cardiotoxicity and other irAEs.
Tapia-orihuela, Ruben
(
University of Miami Miller School of Medicine, Holy Cross Health
, Fort Lauderdale , Florida , United States )
Mark, Justin
(
University of Miami Miller School of Medicine, Holy Cross Health
, Fort Lauderdale , Florida , United States )
Llanos, Alexander
(
University of Miami Miller School of Medicine, Holy Cross Health
, Fort Lauderdale , Florida , United States )
Charnick, Barry
(
PET Imaging Institute of South Florida
, Fort Lauderdale , Florida , United States )
Stone, James
(
MASSACHUSETTS GENERAL HOSPITAL
, Boston , Massachusetts , United States )
Muniz, Jose
(
Cleveland Clinic Florida
, Weston , Florida , United States )
Collado, Elias
(
University of Miami Miller School of Medicine, Holy Cross Health
, Fort Lauderdale , Florida , United States )
Author Disclosures:
Ruben Tapia-Orihuela:DO NOT have relevant financial relationships
| Justin Mark:DO NOT have relevant financial relationships
| Alexander Llanos:No Answer
| BARRY CHARNICK:DO NOT have relevant financial relationships
| James Stone:DO NOT have relevant financial relationships
| Jose Muniz:No Answer
| Elias Collado:DO NOT have relevant financial relationships