Lipoprotein(a) and Metabolic Syndrome are Associated with Increased Risk of Coronary Heart Disease
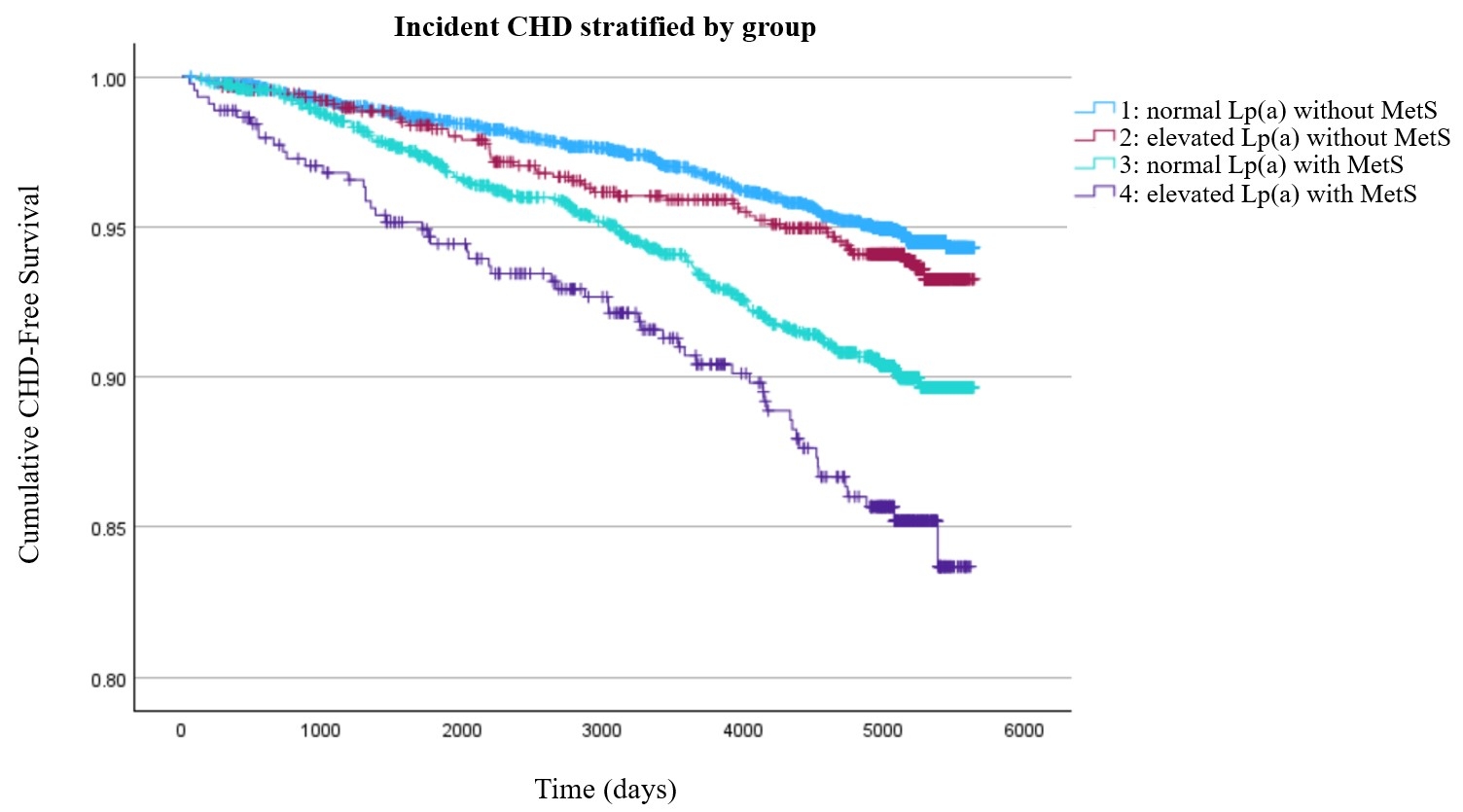
Abstract Body (Do not enter title and authors here): Background Lipoprotein(a) [Lp(a)] and metabolic syndrome (MetS) are well-established risk factors for cardiovascular disease. Recent evidence suggests that high Lp(a) levels may increase the risk of coronary heart disease (CHD) in patients with diabetes, raising the question of whether similar interactions exist between Lp(a) and metabolic syndrome. We aimed to evaluate the joint association of Lp(a) and MetS with incident CHD risk in a large, multi-ethnic, prospective cohort. Methods We analyzed 6,664 participants from the MESA (Multiethnic Study of Atherosclerosis) cohort (median follow-up 14.0 years) without baseline CHD. MetS was defined as ≥3 of the following criteria: waist circumference ≥102 cm (men), or ≥88 cm (women), triglycerides ≥150 mg/dL or use of a fibrate medication, HDL-C <40 (men) or <50 (women) or use of a fibrate medication, SBP ≥130 mm Hg and/or DBP ≥85 mm Hg or use of antihypertensive medication, fasting glucose ≥100 mg/dL or use of antidiabetic medication (4). Elevated Lp(a) was defined as a level ≥50 mg/dL. CHD was defined as myocardial infarction, resuscitated cardiac arrest, or CHD death. Participants were divided into four groups: group 1: Normal Lp(a) without MetS, group 2: elevated Lp(a) without MetS, group 3: normal Lp(a) with MetS, group 4: elevated Lp(a) with MetS. Survival analysis using Kaplan-Meier and multivariable Cox proportional hazard models were performed to assess the relationship between Lp(a), MetS, and time to CHD. Results In an adjusted model, log [Lp(a)] and MetS were both independently associated with CHD (HR: 1.14; 95% CI: 1.03, 1.25) and (HR: 1.75; 95% CI: 1.35, 2.27). Compared to the reference group (normal Lp(a) without MetS), those with elevated Lp(a) without MetS (group 2) did not have increased risk of CHD (HR: 1.30; 95% CI: 0.94, 1.80). However, those with normal Lp(a) with MetS (group 3) had greater risk of CHD (HR: 1.56; 95% CI: 1.18, 2.05). The highest risk for CHD were in those with elevated Lp(a) with MetS (group 4) (HR: 2.37; 95% CI: 1.66, 3.37). Conclusions In this analysis. elevated Lp(a) and MetS independently increase CHD risk. MetS alone significantly increases risk, whereas elevated Lp(a) without MetS does not demonstrate a significant effect. However, their combination confers the highest risk, suggesting a synergistic interaction. These results emphasize the value of assessing Lp(a) in individuals with MetS to improve cardiovascular risk stratification and guide targeted prevention.
Krasner, Joshua
(
University of Miami Miller School of Medicine, Holy Cross Hospital
, Fort Lauderdale , Florida , United States )
Vergara, Carlos
(
Mayo Clinic
, Jacksonville , Florida , United States )
Mark, Justin
(
University of Miami Miller School of Medicine, Holy Cross Hospital
, Fort Lauderdale , Florida , United States )
Lopez, Jose
(
University of Miami Miller School of Medicine, JFK Hospital
, Atlantis , Florida , United States )
Colombo, Rosario
(
University of Miami Miller School of Medicine, Jackson Memorial Hospital
, Miami , Florida , United States )
Yang, Eugene
(
University of Washington
, Seattle , Washington , United States )
Shapiro, Michael
(
Wake Forest Univ School of Medicine
, Winston Salem , North Carolina , United States )
Author Disclosures:
Joshua Krasner:DO NOT have relevant financial relationships
| Carlos Vergara:DO NOT have relevant financial relationships
| Justin Mark:DO NOT have relevant financial relationships
| Jose Lopez:No Answer
| Rosario Colombo:No Answer
| Eugene Yang:DO have relevant financial relationships
;
Advisor:Qure.ai:Past (completed)
; Advisor:Mineralys:Active (exists now)
; Other (please indicate in the box next to the company name):American College of Cardiology:Active (exists now)
; Advisor:Idorsia:Active (exists now)
; Advisor:Genentech:Past (completed)
; Advisor:SkyLabs:Active (exists now)
| Michael Shapiro:DO have relevant financial relationships
;
Consultant:Ionis:Past (completed)
; Consultant:Arrowhead:Past (completed)
; Consultant:Regeneron:Past (completed)
; Researcher:New Amsterdam:Active (exists now)
; Researcher:Merck:Active (exists now)
; Researcher:Novartis:Active (exists now)
; Researcher:Esperion:Active (exists now)
; Researcher:Cleerly:Active (exists now)
; Researcher:Amgen:Active (exists now)
; Consultant:Novo Nordisk:Active (exists now)
; Consultant:Tourmaline:Active (exists now)
; Consultant:Merck:Active (exists now)
; Consultant:New Amsterdam:Past (completed)
; Consultant:Novartis:Active (exists now)