Revisiting the Diabetes Paradox in Aortic Dissection: A Multivariate Analysis from NIS 2022
Abstract Body (Do not enter title and authors here): Background: The role of diabetes mellitus (DM) in Type A aortic dissection (TAAD) mortality is controversial, with some studies suggesting protection and others equating DM to risk factors like hypertension (HTN), hyperlipidemia (HL), smoking, cocaine, and chronic kidney disease (CKD). Using the National Inpatient Sample (NIS) 2022, we assess DM’s impact on TAAD mortality, adjusting for confounders.
Methods: From 32,891,849 hospitalizations, we identified 7,710 TAAD cases (ICD-10: I7100, I71010, I71011) via survey-weighted analyses. DM prevalence was 23.2% (95% CI: 21.0-25.4%); mortality was 12.3% (95% CI: 10.4-14.2%). Mean age was 66.1 years (95% CI: 65.3-66.9), with DM patients older (69.9 years, 95% CI: 68.5-71.2) than non-DM (64.9 years, 95% CI: 64.0-65.9). Females were 40.2% (95% CI: 37.3-43.1%) of non-DM and 44.5% (95% CI: 39.1-50.1%) of DM patients. Non-elective admissions were 6,860 (95% CI: 6,380-7,340); Univariate and multivariate logistic regressions assessed mortality, adjusting for age, HTN, HL, CKD, and a high-risk composite (smoking and cocaine).
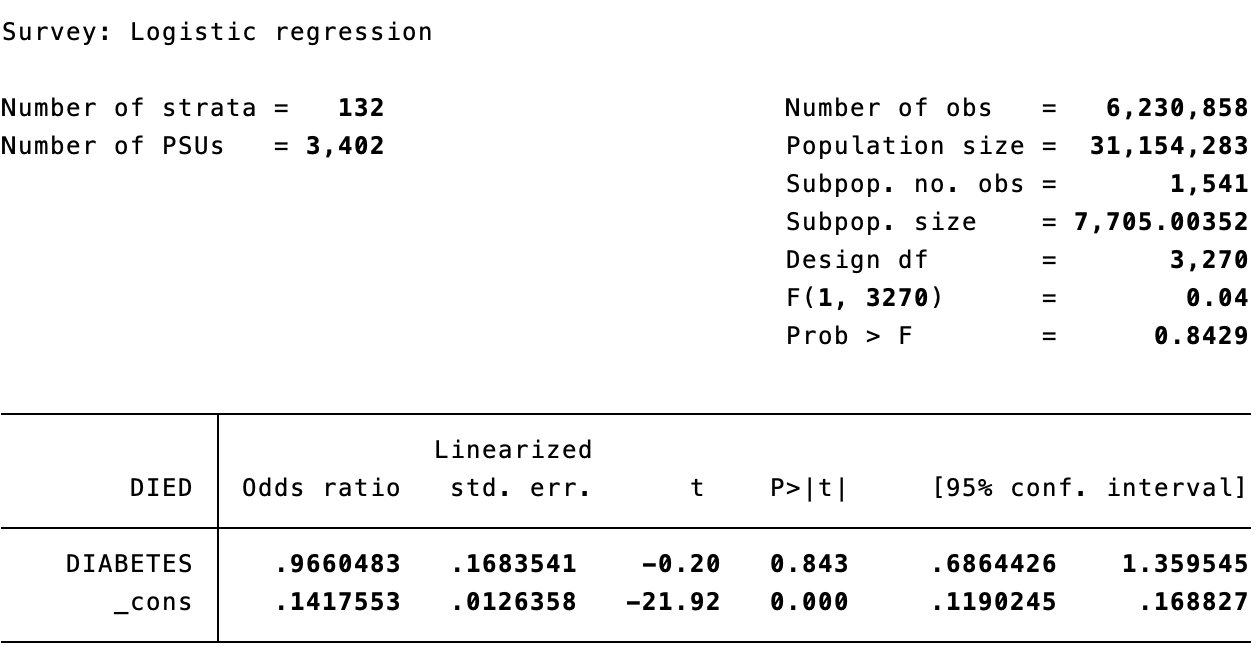
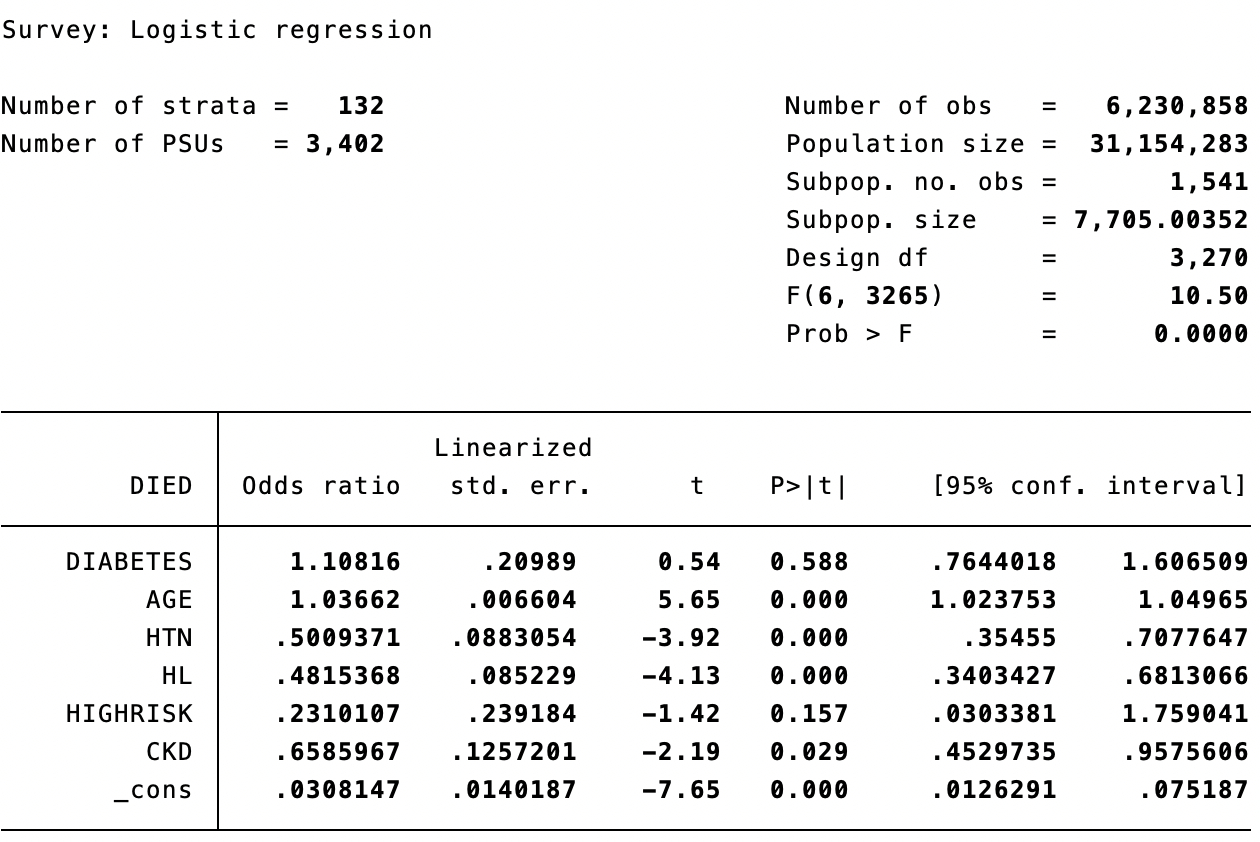
Results: Of 1,541 TAAD patients, 950 died (12.3%, 95% CI: 10.4-14.2%): 735 non-DM (12.7%, 95% CI: 10.6-14.9%) and 215 DM (12.0%, 95% CI: 8.4- 15.6%). Univariate analyses showed no DM-mortality link (OR: 0.966, 95% CI: 0.686-1.360, p=0.843), but age (OR: 1.029, 95% CI: 1.016-1.041, p<0.001), HTN (OR: 0.472, 95% CI: 0.339-0.659, p<0.001), and CKD (OR: 0.670, 95% CI: 0.469- 0.958, p=0.028) predicted mortality; high-risk composite was non-significant (OR: 0.193, p=0.107). Multivariate analysis, adjusting for age, HTN, HL, CKD, and high-risk composite, confirmed DM’s neutrality (OR: 1.108, 95% CI: 0.764-1.607, p=0.588). Age increased mortality (OR: 1.037, 95% CI: 1.024-1.050, p<0.001); HTN (OR: 0.501, 95% CI: 0.355-0.708, p<0.001), HL (OR: 0.482, 95% CI: 0.340- 0.681, p<0.001), and CKD (OR: 0.659, 95% CI: 0.453-0.958, p=0.029) were linked to lower mortality; high-risk composite was non-significant (OR: 0.231, p=0.157).
Conclusions: DM does not affect TAAD mortality, questioning its protective role. Age drives risk, while HTN, HL, and CKD’s lower mortality may reflect optimized management or selection bias, needing further study. Clinicians should focus on age-based risk and HTN/HL management
Janga, Lakshmi Sai Niharika
(
Mount Auburn Hospital
, Cambridge , Massachusetts , United States )
Banga, Akshat
(
Mount Auburn Hospital
, Cambridge , Massachusetts , United States )
Saeed, Muhammad Subhan
(
Mount Auburn Hospital
, Watertown , Massachusetts , United States )
Ying, Xiaonan
(
Mount Auburn Hospital
, Cambridge , Massachusetts , United States )
Nadimpalli, Preethi Meher
(
Rangaraya medical college
, Kakinada , India )
Author Disclosures:
Lakshmi Sai Niharika Janga:DO NOT have relevant financial relationships
| Akshat Banga:DO NOT have relevant financial relationships
| Muhammad Subhan Saeed:DO NOT have relevant financial relationships
| Xiaonan Ying:No Answer
| preethi meher nadimpalli:No Answer