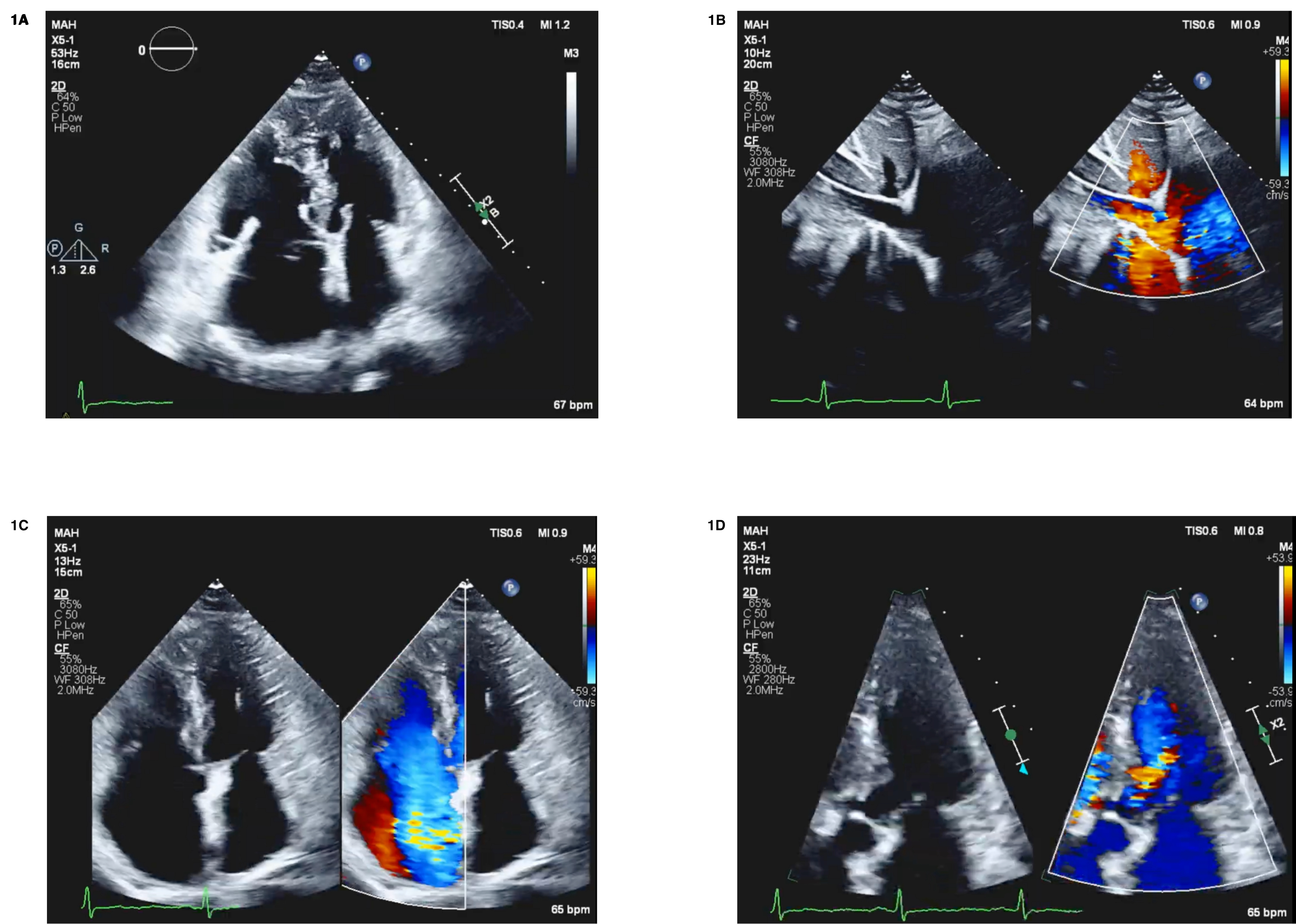
Association Between Right Ventricular-Pulmonary Arterial Coupling and Outcomes in Patients with Heart Failure with Preserved Ejection Fraction
Sherafati Alborz, Dragomirescu Catalin, Brewster Pamela, Kennedy David, Gupta Rajesh, Khouri Samer, Kloster Alex, Manandhar Sareeta, Fares Anas, Aradhyula Vaishnavi, Dube Prabhatchandra, Elzanaty Ahmed, Sajdeya Omar, Khatib-shahidi Bella
BMP10 as novel marker for right atrial dilatation and pressure in precapillary pulmonary hypertension
Llucia-valldeperas Aida, Van Wezenbeek Jessie, Groeneveldt Joanne, Sanchez-duffhues Gonzalo, Vonk Noordegraaf Anton, Bogaard Harm, Goumans Marie Jose, De Man Frances