Endovascular Management of Stanford B Aortic Dissection in a Young Patient with a Thoracoabdominal Aneurysm: A Viable Strategy?
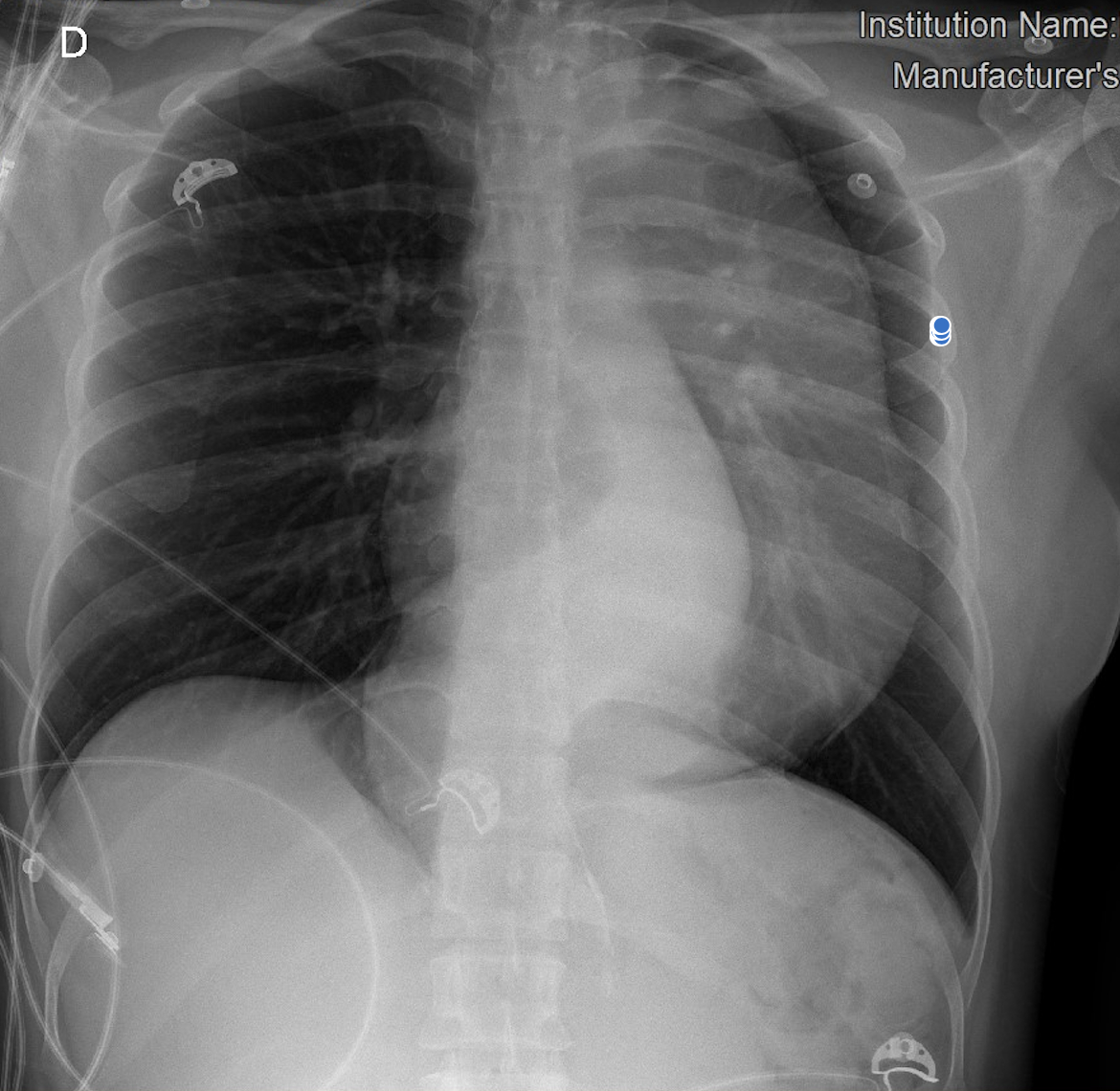
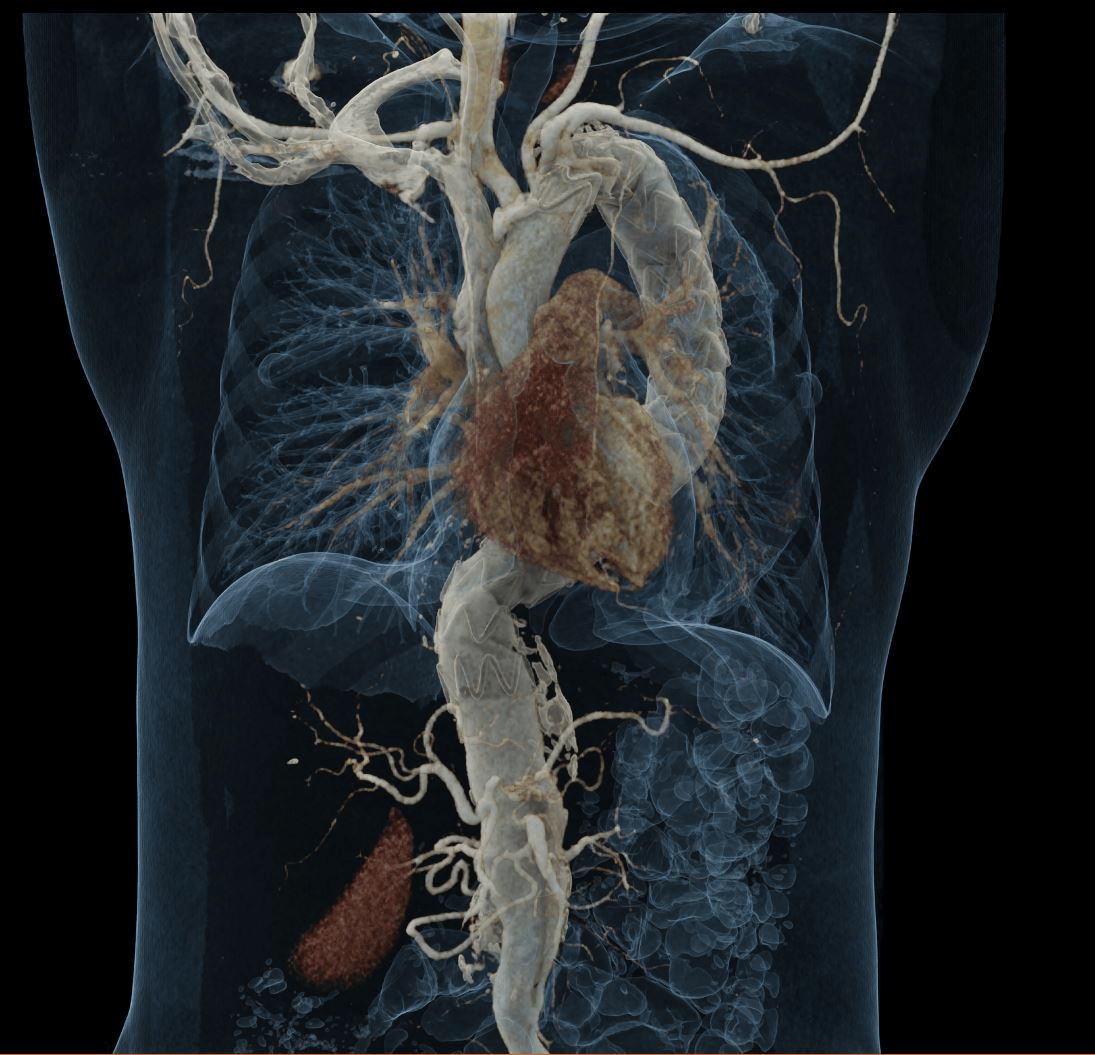
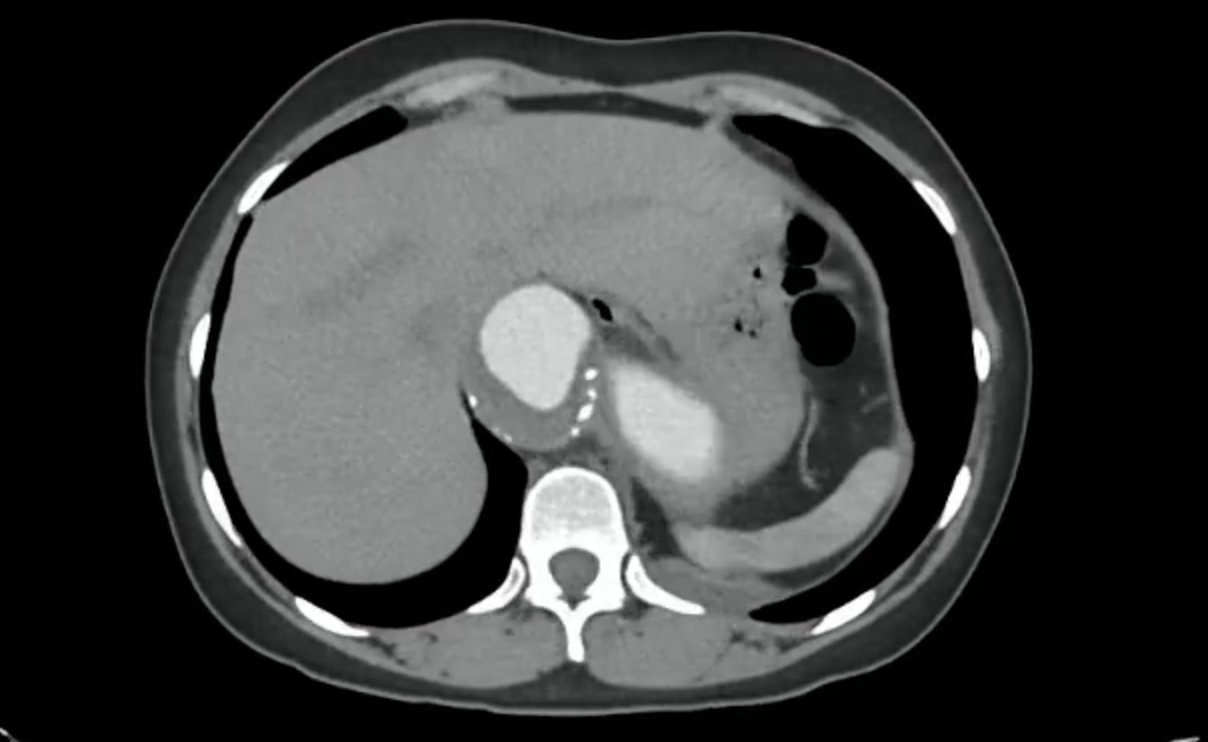
Abstract Body (Do not enter title and authors here): Patient presentation A 35-year-old woman arrived at the emergency department with a five-month history of intermittent interscapular pain, which evolved hours before admission into severe, transfictive left-sided chest pain radiating to the epigastrium, with fatigue and dyspnoea. Physical exam revealed a prominent suprasternal notch mass and bilateral carotid systolic murmurs with thrill. Past medical history included gestational hypertension (2022). Vitals on admission: BP 157/110 mmHg, HR 97 bpm, RR 19, SpO2 91%. Initial workup Chest X-ray showed mediastinal widening. CT angiography revealed a fusiform thoracoabdominal aortic aneurysm (89 × 85 mm, 221 mm length) from T6 to L2, with a dissection flap from the coeliac trunk to the infrarenal segment (Stanford B, DeBakey III), plus intramural thrombus and mural calcifications. A 10 mm flap in the proximal coeliac trunk and an intimal tear at the origin of the left subclavian artery (extending 54 mm) were also seen. Additional findings: left pleural effusion and hepatic haemangiomas. Diagnosis and management Diagnosis: thoracoabdominal aneurysm with Stanford B, DeBakey IIB dissection. Medical management: IV nitroprusside, esmolol, and analgesia. Due to high rupture risk, endovascular repair was chosen over open surgery. Via right femoral access, two endografts were deployed in the thoracic/abdominal aorta. The left subclavian artery, arising from the false lumen, was not fenestrated. The procedure involved bleeding requiring transfusion, but no further complications. Follow-up Three days later, the patient presented abdominal pain and hemoglobin drop. CT suggested a type IA endoleak, sealed endovascularly. A left carotid-subclavian bypass was later performed. Echocardiogram revealed a bicuspid aortic valve with moderate regurgitation. After 12 days, the patient was discharged in improvement, on beta-blocker and antiplatelet therapy, and continues follow-up. Conclusion This case highlights the importance of early diagnosis and tailored management of Stanford B dissection with thoracoabdominal aneurysm in young patients. Bicuspid valve anatomy predisposes to aortic disease, requiring close surveillance. Despite ongoing debate, TEVAR proved effective here, especially in experienced hybrid centers.
Maldonado May, Ana Cristina
(
Instituto Nacional de Cardiologia
, Mexico , Mexico )
Berrio Becerra, Carla Angelica
(
Instituto Nacional de Cardiologia
, Ciudad de Mexico , Mexico )
Barrón, Alejandro
(
Instituto Nacional de Cardiologia
, Mexico , Mexico )
Santillán, Sofía
(
Instituto Nacional de Cardiologia
, Mexico , Mexico )
Esquivel, Martin
(
Instituto Nacional de Cardiologia
, Mexico , Mexico )
Berumen Barreto, Jesus Emilio
(
Autonomous University of Queretaro
, Queretaro , Mexico )
Miranda Corona, Maria Fernanda
(
Instituto Nacional de Cardiologia
, Mexico , Mexico )
Arias-mendoza, Alexandra
(
Instituto Nacional de Cardiologia
, Mexico , Mexico )
Araiza, Diego
(
Instituto Nacional de Cardiologia
, Ciudad de Mexico , Mexico )
Author Disclosures:
Ana Cristina Maldonado May:DO NOT have relevant financial relationships
| Carla Angelica Berrio Becerra:DO NOT have relevant financial relationships
| Alejandro Barrón:DO NOT have relevant financial relationships
| Sofía Santillán:No Answer
| Martin Esquivel:No Answer
| Jesus Emilio Berumen Barreto:DO NOT have relevant financial relationships
| Maria Fernanda Miranda Corona:DO NOT have relevant financial relationships
| Alexandra Arias-Mendoza:No Answer
| Diego Araiza:No Answer
Berumen Barreto Jesus Emilio, Escobar Rios Marc Antoine, Miranda Corona Maria Fernanda, Esquivel Martin, Maldonado May Ana Cristina, Berrio Carla, Araiza Diego
4370167_File000000.jpg
4370167_File000001.jpg
4370167_File000002.jpg
You have to be authorized to contact abstract author. Please, Login