Center-Based, Home-Based, and Technology-Enhanced Cardiac Rehabilitation Equally Reduce Mortality Risk in Veterans
Abstract Body (Do not enter title and authors here): Introduction: Cardiac rehabilitation (CR) is a class I recommendation following a cardiac event, yet fewer than 20% of eligible patients enroll. Home-based CR (HBCR), especially when enhanced with mobile health tools like fitness trackers and smartphones to increase engagement—termed technology-enabled CR (TECR)—may improve outcomes. We hypothesized that TECR, HBCR (without technology), and center-based CR (CBCR) be associated with lower mortality compared to usual care, with TECR conferring the greatest benefit.
Methods: We studied veterans referred to CR at the Atlanta VA Healthcare System from January 1, 2017, to June 1, 2022. Patients chose TECR, HBCR alone, or CBCR under shared decision-making. Usual care consisted of patients who did not enroll in any CR. Clinical and mortality data were obtained from the VA Corporate Data Warehouse with MDClone, a self-service data analytics platform. We excluded those who died or were lost to follow-up within 30 days of referral and used inverse probability of treatment weighting (IPTW) to balance baseline characteristics.
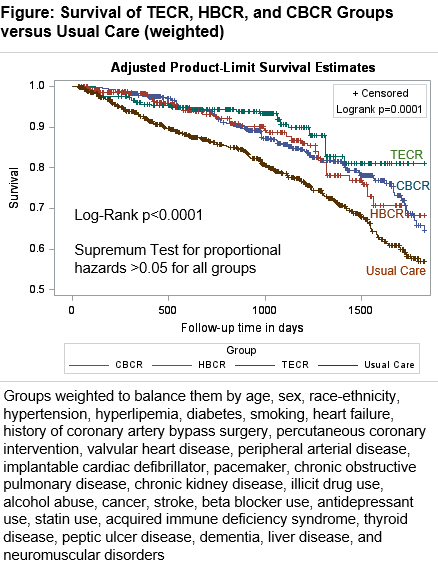
Results: Among 1,755 referred veterans (mean age 65 [SD 10] years; 50% Black; 6% women), pre-pandemic enrollment before March 16th, 2020, was 15% TECR, 11% HBCR, 33% CBCR, and 41% usual care. Afterwards, HBCR enrollment increased to 30%, CBCR fell to 15%, and others remained stable. After IPTW adjustment, baseline characteristics were well balanced. Over a mean (SD) follow-up of 2.6 (1.5) years, 333 veterans (19%) died. Adjusted hazard ratios for mortality versus usual care were: TECR 0.41 (95% CI, 0.27–0.65), HBCR 0.61 (0.44–0.84), and CBCR 0.56 (0.42–0.73). The TECR estimate was the lowest, but did not significantly differ from HBCR (p=0.14) or CBCR (p=0.21).
Conclusions: All CR formats were associated with lower mortality compared to usual care. Technology-enabled CR may offer additional benefit, but larger randomized trials are needed to determine its comparative effectiveness.
Shah, Amit
(
EMORY UNIVERSITY
, Atlanta , Georgia , United States )
Li, Louis
(
EMORY UNIVERSITY
, Atlanta , Georgia , United States )
Aggarwal, Vinod
(
VHA Office of Healthcare Innovation and Learning, VA Central Office
, Washington , District of Columbia , United States )
Zafari, Abarmard
(
EMORY UNIVERSITY
, Atlanta , Georgia , United States )
Park, Linda
(
UCSF
, San Francisco , California , United States )
Harzand, Arash
(
Atlanta VA Medical Center
, Decatur , Georgia , United States )
Author Disclosures:
Amit Shah:DO NOT have relevant financial relationships
| Louis Li:DO NOT have relevant financial relationships
| Vinod Aggarwal:DO NOT have relevant financial relationships
| Abarmard Zafari:DO NOT have relevant financial relationships
| Linda Park:DO NOT have relevant financial relationships
| Arash Harzand:DO NOT have relevant financial relationships