Vascular Imaging for ASCVD Risk Stratification: Predictive Value of Carotid Plaque, Coronary Artery Calcium, and Retinal Biomarker (Dr.Noon CVD)
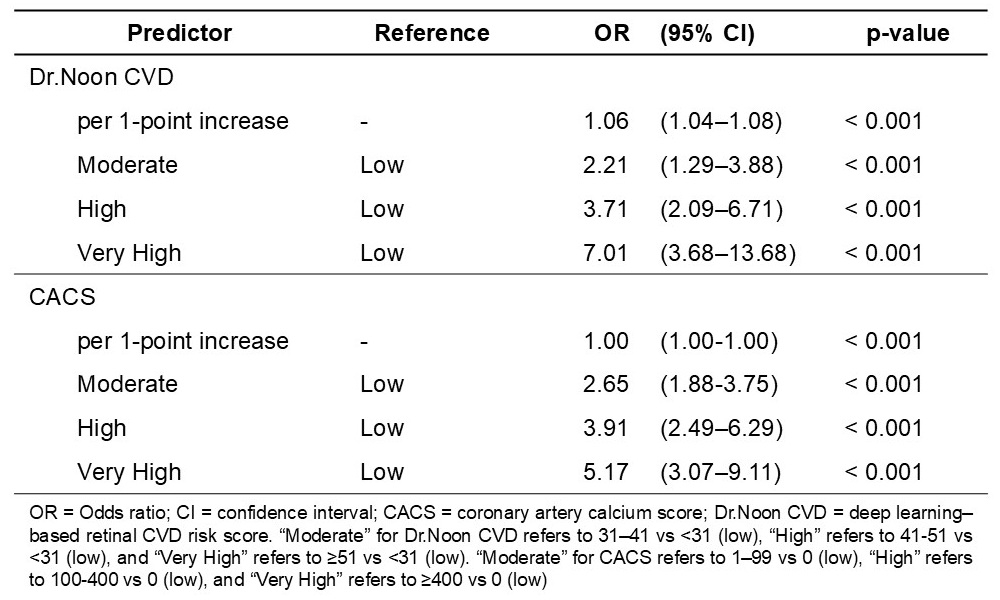
Abstract Body (Do not enter title and authors here): Background Carotid ultrasound is convenient and widely used for CVD risk assessment. Plaques—especially in the internal carotid artery (ICA) or bulb—predict atherosclerotic cardiovascular disease (ASCVD) events, but plaque burden alone may miss vascular vulnerability or microvascular disease; additional biomarkers are needed to refine risk prediction. Hypothesis We hypothesized that coronary artery calcium score (CACS) and a deep learning–based retinal biomarker (Dr.Noon CVD) would each associate with carotid plaque and predict ASCVD events, independently and in combination. Methods We analyzed 1,075 high-risk adults from the CMERC-HI cohort with carotid ultrasound, CACS, and Dr.Noon CVD scores. Plaque was defined as any ICA/bulb lesion. ASCVD events (nonfatal or fatal) included stroke, heart failure, and myocardial infarction, and cardiovascular deaths. Age- and sex-adjusted logistic regression assessed associations of plaque with CACS (low: 0; moderate: 1–99; high: 100-400, very high: ≥400) and Dr.Noon CVD (low: <31; moderate: 31-40; high: 41-50; very high: ≥51). For ASCVD event prediction, Cox models compared high and very high vs. low+moderate for CACS and Dr.Noon CVD, and plaque presence vs. absence. Performance was evaluated using hazard ratios (HRs), C-indices, and Kaplan–Meier curves. Results Plaque was present in 719 (66.8%) participants. Over 8.8 years (median), 72 ASCVD events occurred. Incidence rates ranged from 0–14.6 per 1,000 PYs (Dr.Noon CVD), 2.6–19.7 per 1,000 PYs (CACS), and 5.6–9.3 per 1,000 PYs (plaque). Each 1-point Dr.Noon CVD increase was associated with plaque (OR 1.06; 95% CI 1.04–1.08; p<0.001). Participants at moderate, high, and very high Dr.Noon CVD risk had ORs of 2.21, 3.71, and 7.01 for plaque (all p<0.001). Similar trends were seen for CACS: moderate, high, and very high categories had ORs of 2.65, 3.91, and 5.17, respectively (all p<0.001). In Cox models, the C-index was 0.680 for Dr.Noon CVD, 0.676 for CACS, and 0.661 for plaque alone. Combining plaque with Dr.Noon CVD or with CACS improved the C-index by Δ +0.060 and +0.038 versus plaque only (both p<0.001). Kaplan–Meier curves confirmed clear risk stratification (log-rank p<0.001). Conclusion Dr.Noon CVD and CACS each associate with carotid plaque and predict ASCVD events. The greatest improvement in discrimination occurred when combining Dr.Noon CVD with plaque, underscoring its potential for practical vascular risk stratification.
Cho, Jungkyung
(
Mediwhale
, Seoul , Korea (the Republic of) )
Park, Junseok
(
Mediwhale
, Seoul , Korea (the Republic of) )
Nam, Dongjin
(
Severance Hospital
, Seoul , Korea (the Republic of) )
Thakur Sahil, Seo Jaewon, Park Tae Hyun, Kim Hyeonmin, Arora Vinay, Nusinovici Simon, Rim Tyler, Rastogi Sparsh, Modi Khushboo, Rukmini A.v., Kim Sunwoong, Seo Wonyoung, Park Junseok, Nam Dongjin, Cho Jungkyung