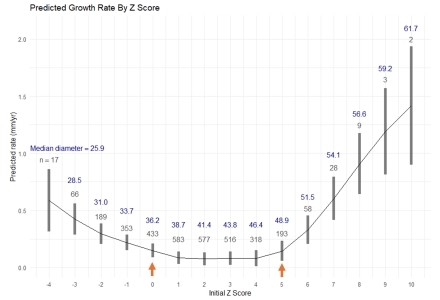
Abstract Body (Do not enter title and authors here): Background Predicting ascending aortic growth remains challenging, with few robust clinical predictors beyond known genetic aortopathies. Most current models assume linear growth and assess change over the longest available imaging interval. While convenient, these methods may miss plausible non-linear relationships between size and growth, especially in the context of known compensatory wall remodeling. Research question Are there non-linear associations between baseline ascending aortic diameter—indexed for body size, age, and sex—and future aortic growth? Methods We conducted a single-center, retrospective study of patients with ≥2 chest CT/MR angiograms and double-oblique measurements of the mid-ascending aorta. Z-scores normalized aortic diameter by sex, age, and body surface area. Generalized Additive Models (GAMs) with smoothing splines were used to predict aortic growth based on baseline characteristics (maximal diameter, demographics, and clinical risk factors including hypertension, smoking status, and Marfan syndrome). Results Among 3,349 patients (11,840 scans; 15,103 person-years of follow-up), mean age was 61 ± 13 years; 68% were male; 85% had hypertension; and 2.6% had Marfan syndrome. Both linear models and initial GAMs using clinical variables showed limited predictive power (R2 < 0.01). However, baseline Z-score exhibited a significant non-linear relationship with future growth (Figure 1), with two inflection points (arrows): one below Z = 0 (~36 mm) and another above Z = 5 (~49 mm). This relationship persisted after excluding patients with known genetic aortopathy. Conclusion Indexed baseline aortic size is non-linearly associated with future ascending aortic growth rate, likely in a quadratic fashion. While accelerated growth was observed above surgical thresholds (Z > 5, diameter > ~49 mm), fast growth also occurred at “normal” aortic sizes (Z < 0, diameter < ~36 mm), a range that accounts for ~1/3 of type A dissections. These findings highlight both the indolent nature of mild-moderate dilation (Z = +2–+5) and the shortcomings of current surveillance strategies, which often overlook patients with rapid growth at non-dilated sizes—underscoring the need for non-size-based risk metrics such as aortic shape, wall biology, and genetics.
Marway, Prabhvir
(
University of Michigan
, Ann Arbor , Michigan , United States )
Campello Jorge, Carlos Alberto
(
University of Michigan
, Ann Arbor , Michigan , United States )
Spahlinger, Greg
(
University of Wisconsin
, Southfield , Michigan , United States )
Knauer, Heather
(
University of Michigan
, Ann Arbor , Michigan , United States )
Hofmann Bowman, Marion
(
University of Michigan
, Ann Arbor , Michigan , United States )
Murthy, Venkatesh
(
University of Michigan
, Ann Arbor , Michigan , United States )
Burris, Nicholas
(
University of Wisconsin-Madison
, Madison , Wisconsin , United States )
Author Disclosures:
Prabhvir Marway:DO NOT have relevant financial relationships
| Carlos Alberto Campello Jorge:No Answer
| Greg Spahlinger:DO NOT have relevant financial relationships
| Heather Knauer:DO have relevant financial relationships
;
Royalties/Patent Beneficiary:Imbio Inc:Active (exists now)
| Marion Hofmann Bowman:DO NOT have relevant financial relationships
| Venkatesh Murthy:No Answer
| Nicholas Burris:DO have relevant financial relationships
;
Royalties/Patent Beneficiary:Imbio Inc:Active (exists now)