A novel risk score predicts the prevalence of left atrial low-voltage areas and rhythm outcome in patients undergoing long-standing persistent atrial fibrillation ablation
Ooka Hirotaka, Nakao Sho, Kusuda Masaya, Ariyasu Wataru, Kudo Satoshi, Fujii Subaru, Mano Toshiaki, Matsuda Yasuhiro, Masuda Masaharu, Okamoto Shin, Ishihara Takayuki, Nanto Kiyonori, Tsujimura Takuya, Hata Yosuke, Uematsu Hiroyuki
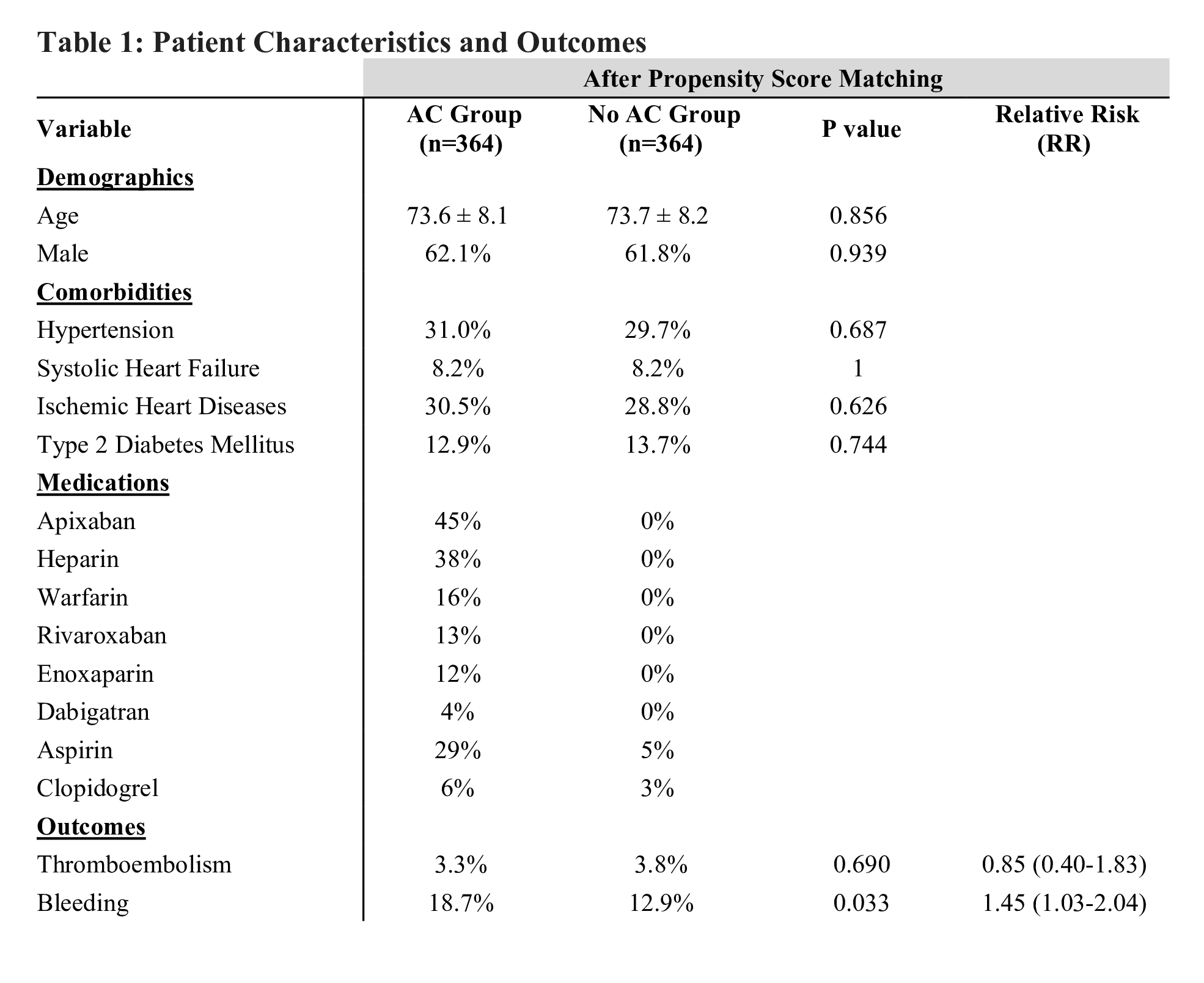
4-5 Years Outcomes of Left Atrial Appendage Closure vs. Oral Anticoagulants in Atrial Fibrillation: A Systematic Review and Meta-Analysis:
Khan Muhammad Aslam, Haider Taimoor, Bhattarai Shraddha, Afzal Hafsa, Khan Bilal, Muhammad Anza, Shafique Nouman, Bhatia Hitesh, Aafreen Asna, Adil Abid Nawaz Khan, Akbar Usman, Khan Alamzaib, Haider Muhammad Adnan