A Hidden Threat: Trazodone-Induced Warfarin Failure Leading to Acute Mechanical Aortic Valve Thrombosis
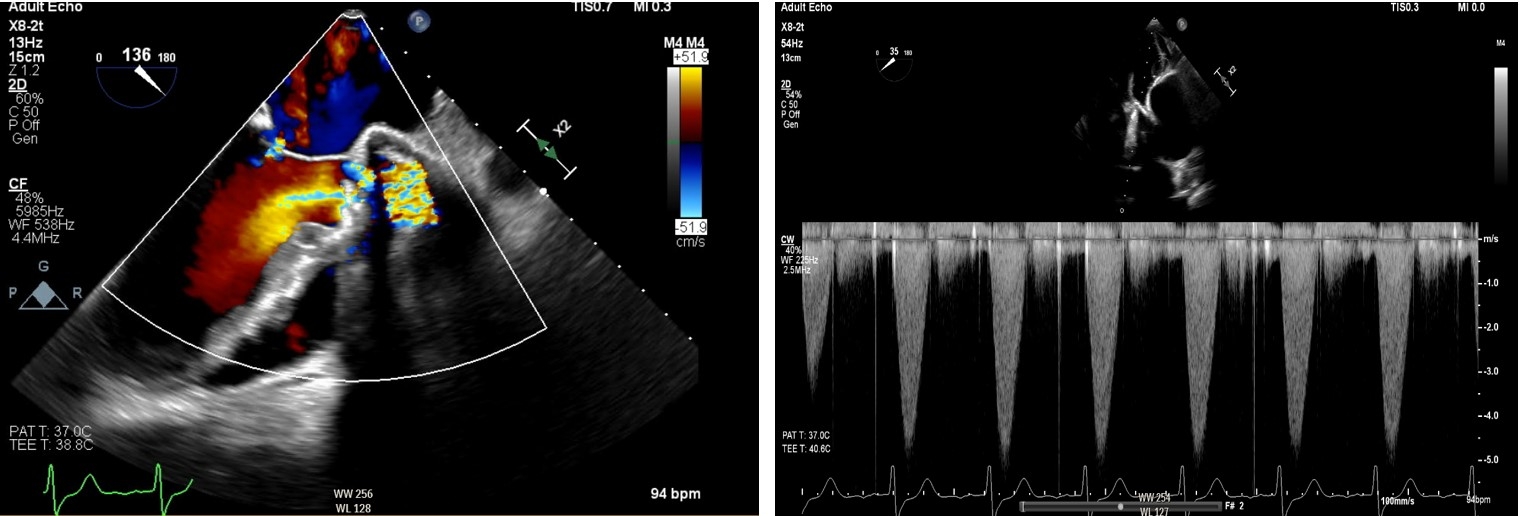
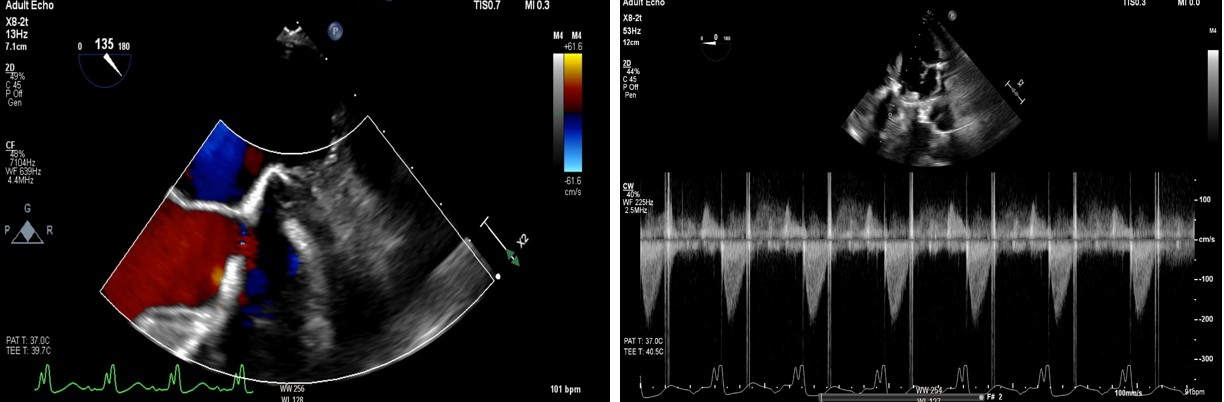
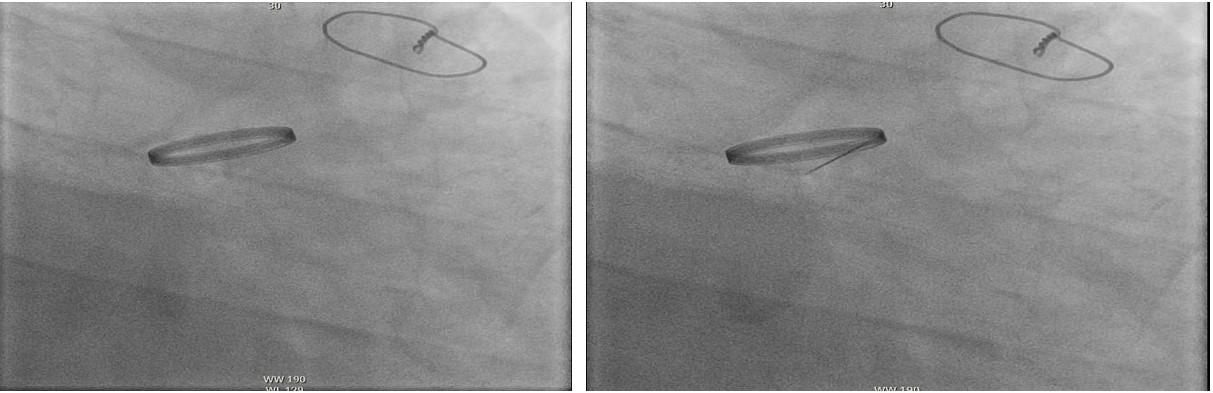
Abstract Body (Do not enter title and authors here): Background: Warfarin remains essential for preventing thrombosis in patients with mechanical heart valves. However, its narrow therapeutic index and susceptibility to drug interactions demand careful monitoring. We present a case of subacute mechanical aortic valve thrombosis likely precipitated by a warfarin–trazodone interaction. Case Presentation: A 58-year-old man with a history of bicuspid aortic stenosis requiring mechanical valve replacement—previously stable on chronic warfarin therapy (5 mg daily)—presented to the ED with three days of worsening dyspnea, cough, and upper back pain. Upon arrival, he was hypertensive, hypoxic, and in respiratory distress, exhibiting cold extremities, bilateral crackles, and an audible mechanical valve click. Labs revealed an INR of 1.3 (previously therapeutic), lactate 9.0 mmol/L, troponin 233 ng/L, and BNP 6812 pg/mL. CTA showed possible multifocal pneumonia. Initially, he was diagnosed with septic shock and ARDS, requiring vasopressors and BiPAP. Shortly after, he suffered a cardiac arrest, requiring intubation and vasopressor escalation. Transthoracic echocardiography (TTE) revealed a peak gradient of 3.7 m/s and mean gradient of 28 mmHg across the prosthetic valve. Urgent transesophageal echocardiography (TEE) showed severely restricted leaflet motion with torrential aortic regurgitation—highly suggestive of valve thrombosis. Due to prohibitive surgical risk, thrombolysis with alteplase (25 mg over 6 hours) was administered. Repeat TEE demonstrated improved leaflet motion (velocity 2.2 m/s, mean gradient 17.6 mmHg), LVEF of 25%, and new severe mitral regurgitation. He was stabilized on milrinone and extubated by hospital day five. Despite restarting warfarin—at doses up to 30 mg daily (three times his prior regimen)—therapeutic INR was not achieved until 10 days later. Further interrogation revealed, thirteen days prior to ED visit, he was started on trazodone 50 mg. No other interacting medications or hepatic dysfunction were identified. Trazodone was identified as the likely culprit and had been discontinued. His INR subsequently normalized. Discussion: Trazodone may reduce warfarin efficacy, leading to subtherapeutic INR and valve thrombosis in mechanical valve patients. While the exact mechanism is unclear, proposed theories include CYP2C9 induction, increased warfarin clearance, or protein-binding displacement. This case highlights the need for close INR monitoring when initiating trazodone in patients on warfarin.
Vogt, Cody
(
Geisinger Medical Center
, Danville , Pennsylvania , United States )
Malik, Saad
(
Geisinger Medical Center
, Danville , Pennsylvania , United States )
Pfirman, Kristopher
(
Geisinger Medical Center
, Danville , Pennsylvania , United States )
Author Disclosures:
Cody Vogt:DO NOT have relevant financial relationships
| Saad Malik:DO NOT have relevant financial relationships
| Kristopher Pfirman:DO NOT have relevant financial relationships