Effects of Device-Measured Physical Activity on Disease Progression and Cardiovascular Outcomes in Phenotype-Negative Carriers of Cardiomyopathy-Associated Rare Variants
Abstract Body (Do not enter title and authors here): Background: Exercise may lead to disease progression and higher risk of sudden death in certain cardiomyopathies conferred by rare genetic variants. Whether general activity recommendations (i.e.,150-300 minutes/week of moderate-to-vigorous physical activity (MVPA)] are appropriate for individuals carrying a cardiomyopathy-associated variant without overt disease (G+P-) are unclear.
Research Question: Do the effects of MVPA on cardiovascular (CV) outcomes, cardiac structure and function, and risk of developing overt cardiomyopathy and arrhythmias vary according to G+P- status?
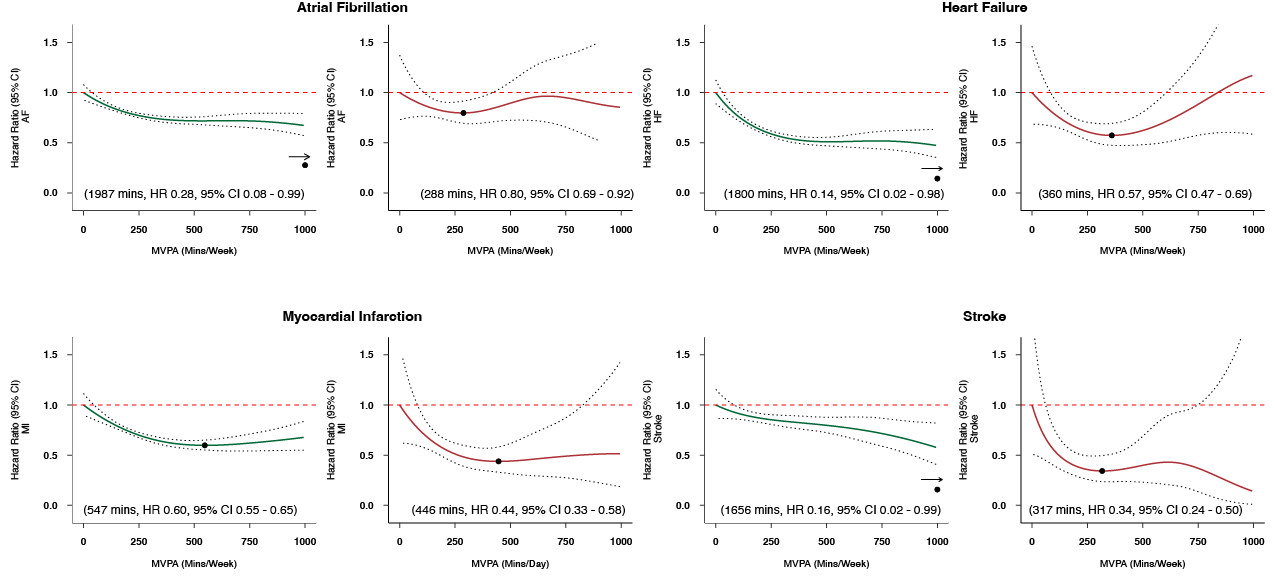
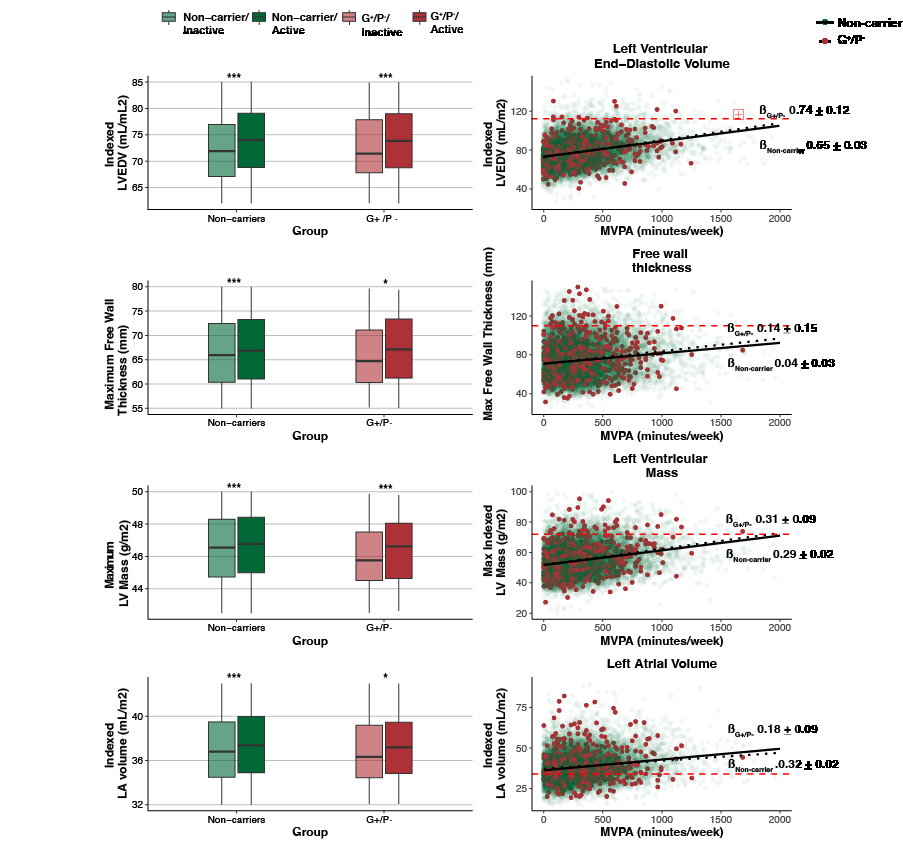
Methods: In UK Biobank participants undergoing 1-week of accelerometry, we assessed: i) associations between MVPA (as a spline term) and incident CV outcomes (i.e.,atrial fibrillation [AF], heart failure [HF], myocardial infarction [MI], and stroke) using Cox models adjusted for demographic and lifestyle factors, deriving optimal levels of MVPA from splines for each outcome; ii) effects of MVPA on derived indices of cardiac structure and function in a subset with cardiac magnetic resonance (CMR) imaging; iii) effects on progression to overt cardiomyopathy and malignant arrhythmia using analogous models estimating risk of incident non-ischemic cardiomyopathy (NICM) and ventricular arrhythmias (VA). The presence of varying effects on account of G+P- status was assessed by comparing model results with non-carriers.
Results: Among 84,733 individuals (age 62±8 years, 56.4% women, 3,986 G+P-) undergoing accelerometry, MVPA levels were nearly identical for G+P- individuals and non-carriers (both medians:230, quartile-1:115, quartile-3:403). In multivariable models, higher MVPA was broadly associated with lower risk of incident CV disease in the G+P- group (hazard ratio[HR] at optimal MVPA level vs zero, 95% CI, AF:0.80, 0.69–0.92; HF:0.57, 0.47–0.69; MI:0.44, 0.33–0.58; stroke:0.34,0.24–0.50]) (Figure 1). MVPA was also associated with similar degrees of cardiac remodeling (e.g., LV dilation) in G+P- vs non-carriers (Figure 2). No associations were observed between MVPA and risk of NICM or VA in G+P- individuals.
Conclusions and Relevance: MVPA generally within the range of guideline-based recommendations associates with lower risk of adverse CV outcomes and similar degrees of cardiac remodeling for G+P- individuals compared to non-carriers. Although individual-level risk stratification remains critical, G+P- individuals should be encouraged to adhere to guideline-based activity recommendations.
Ajufo, Ezimamaka
(
Brigham and Womens Hospital
, Boston , Massachusetts , United States )
Kany, Shinwan
(
Broad Institute
, Cambridge , Massachusetts , United States )
Jurgens, Sean
(
Broad Institute and Amsterdam UMC
, Amsterdam , Netherlands )
Churchill, Timothy
(
Massachusetts General Hospital
, Boston , Massachusetts , United States )
Guseh, James
(
Massachusetts General Hospital
, Boston , Massachusetts , United States )
Aragam, Krishna
(
Massachusetts General Hospital
, Boston , Massachusetts , United States )
Nauffal, Victor
(
Brigham and Women's Hospital
, Boston , Massachusetts , United States )
Pirruccello, James
(
UCSF Division of Cardiology
, San Francisco , California , United States )
Choi, Seung Hoan
(
Boston University
, Boston , Massachusetts , United States )
Lakdawala, Neal
(
Brigham and Womens Hospital
, Boston , Massachusetts , United States )
Ho, Carolyn
(
Brigham and Womens Hospital
, Brookline , Massachusetts , United States )
Khurshid, Shaan
(
Massachusetts General Hospital
, Boston , Massachusetts , United States )
Ellinor, Patrick
(
Massachusetts General Hospital
, Boston , Massachusetts , United States )
Author Disclosures:
Ezimamaka Ajufo:DO NOT have relevant financial relationships
| Neal Lakdawala:DO have relevant financial relationships
;
Consultant:BMS:Active (exists now)
; Advisor:Neuvocore:Active (exists now)
; Consultant:Gemma:Active (exists now)
; Advisor:Kardigan:Active (exists now)
; Consultant:Tenaya:Active (exists now)
; Consultant:Cytokinetics:Active (exists now)
; Consultant:Pfizer:Past (completed)
; Consultant:Alexion:Active (exists now)
| Carolyn Ho:DO have relevant financial relationships
;
Consultant:Bristol Myers Squibb:Active (exists now)
; Researcher:Tenaya:Active (exists now)
; Consultant:Tenaya:Active (exists now)
; Research Funding (PI or named investigator):Biomarin:Past (completed)
; Research Funding (PI or named investigator):Lexicon:Active (exists now)
; Research Funding (PI or named investigator):Cytokinetics:Active (exists now)
; Research Funding (PI or named investigator):Bristol Myers Squib:Active (exists now)
; Consultant:Novo Nordisk:Active (exists now)
; Consultant:Bayer:Active (exists now)
; Consultant:Sanofi:Past (completed)
; Consultant:Biomarin:Past (completed)
; Consultant:Lexicon:Active (exists now)
; Consultant:Cytokinetics:Active (exists now)
| Shaan Khurshid:No Answer
| Patrick Ellinor:No Answer
| Shinwan Kany:DO NOT have relevant financial relationships
| Sean Jurgens:DO NOT have relevant financial relationships
| Timothy Churchill:No Answer
| James Guseh:No Answer
| Krishna Aragam:No Answer
| Victor Nauffal:DO have relevant financial relationships
;
Consultant:Abbott:Past (completed)
; Research Funding (PI or named investigator):Novo Nordisk:Active (exists now)
| James Pirruccello:DO have relevant financial relationships
;
Other (please indicate in the box next to the company name):JACC:Active (exists now)
| Seung Hoan Choi:DO NOT have relevant financial relationships