Risk of Gastrointestinal Bleeding by Mechanical Circulatory Support Device
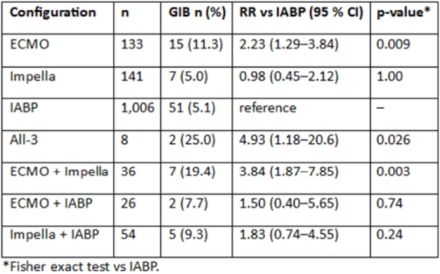
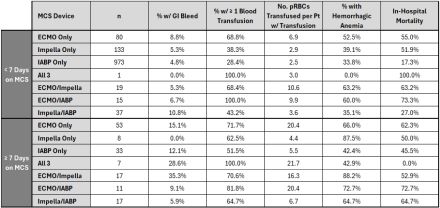
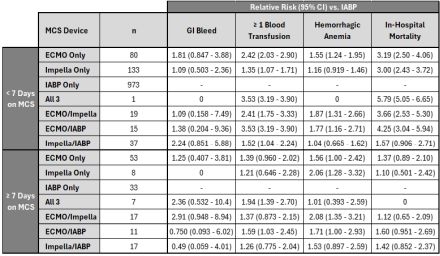
Abstract Body (Do not enter title and authors here): Introduction Gastrointestinal bleeding (GIB) is a common, potentially modifiable, complication in patients receiving mechanical circulatory support (MCS) but head-to-head data for single and multi-device MCS strategies remains sparse. Research Question To compare the incidence of GIB, transfusion burden, and in-hospital mortality across single- and multi-device MCS strategies using the MIMIC-IV critical care database. Methods This retrospective study analyzed ICU encounters (2009-2022) of adults at Beth Israel Deaconess Medical Center with documented Extracorporeal Membranous Oxygen (ECMO), Impella, or Intra-aortic Balloon Pump (IABP) use. Data was obtained using the MIMIC-IV database with 85,000 ICU encounters. Exposures were categorized as single-device (ECMO, Impella, IABP) or multi-device combinations. The primary endpoint was any GIB (ICD-9/10 diagnoses). Secondary endpoints were packed red-blood-cell (pRBC) transfusion, hemorrhagic anemia, and in-hospital mortality. Categorical variables were compared using Fisher’s exact test; relative risks (RR) with 95% confidence intervals (CI) were calculated in comparison to IABP. Further analyses were stratified by support duration (<7 vs. ≥7 days). Results A total of 1,404 MCS encounters were analyzed. Among 1,280 single-device ICU admissions (IABP=1,006, Impella=141, ECMO=133) GIB occurred in 5.1%, 5.0%, and 11%, respectively. ECMO had 2.2x higher risk vs. IABP (p<.01) and 2.3x vs. Impella (p=0.07). When limited to patients supported for <7 days, the risk of GIB on ECMO vs. IABP narrowed to 1.8 (95% CI 0.85-3.9), but the risk of need for pRBC transfusion or hemorrhagic anemia remained 2.4 (95% CI 2.0-2.9) and 1.6 (95% CI 1.2-2.0) times higher, respectively. pRBC units per transfused patient was likewise greatest at both durations with ECMO (6.9, 20.4) vs. Impella (2.9, 4.4) and IABP (2.5, 5.5). Multi-device cases showed higher crude bleeding (19–25%) but small sample size and heterogeneous timing or sequencing limit inference. In-hospital mortality likely reflected underlying severity of illness, with single-device ECMO and Impella both exceeding 50% vs.18% for IABP. Conclusions Gastrointestinal bleeding and transfusion burden vary significantly by MCS strategy and duration, with ECMO carrying the greatest risk. Bleeding risk should factor into MCS selection. Prospective studies are needed to evaluate individualized bleeding mitigation protocols.
Khalid, Abdullah
(
Tufts Medical Center
, Boston , Massachusetts , United States )
Khullar, Rohit
(
Tufts Medical Center
, Boston , Massachusetts , United States )
Kini, Saurav
(
Tufts Medical Center
, Boston , Massachusetts , United States )
Philip, Anil
(
John H Stroger of Cook County
, Chicago , Illinois , United States )
Chweich, Haval
(
Tufts Medical Center
, Boston , Massachusetts , United States )
Author Disclosures:
Abdullah Khalid:DO NOT have relevant financial relationships
| Rohit Khullar:DO NOT have relevant financial relationships
| Saurav Kini:DO NOT have relevant financial relationships
| Anil Philip:DO NOT have relevant financial relationships
| Haval Chweich:No Answer
Philip Anil, Banga Akshat, Saeed Muhammad Subhan, Briones-zamora Killen H., Briones-claudett Killen H., Kohli Saksham, Khullar Rohit, George Lina James, Mautong Hans, John Kevin, Varma Revati, Kini Saurav, Khalid Abdullah, Saha Shubhashis, Caputi Zuniga Angelo
4367162_File000000.jpg
4367162_File000001.jpg
4367162_File000002.jpg
You have to be authorized to contact abstract author. Please, Login