Oral Anticoagulant Monotherapy vs Dual Antithrombotic Therapy in Patients with Atrial Fibrillation and Stable Coronary Artery Disease Following Percutaneous Coronary Intervention: Insights from a Real-World TriNetX Cohort Study
Abstract Body (Do not enter title and authors here): Background: The optimal long-term antithrombotic strategy in patients with atrial fibrillation (AF) and stable coronary artery disease (CAD) post-percutaneous coronary intervention (PCI) remains uncertain. While oral anticoagulant (OAC) monotherapy may reduce bleeding risk, concerns persist regarding its effectiveness in preventing ischemic events compared to combined OAC and single antiplatelet therapy (SAPT).
Aim: This study aimed to compare the effectiveness and safety of OAC monotherapy versus combined OAC and SAPT in a real-world cohort of patients with AF and stable CAD, ≥1 year post-PCI.
Methods: Using the TriNetX global federated health research network, we conducted a retrospective cohort analysis including 6,950 matched patients on OAC monotherapy and 6,950 matched patients on combined OAC and SAPT, after propensity score matching from initial cohorts of 10,304 and 8,235 patients, respectively. Outcomes evaluated at 1 and 3 years included all-cause mortality, ischemic stroke, myocardial infarction (MI), pulmonary embolism (PE), and major bleeding events.
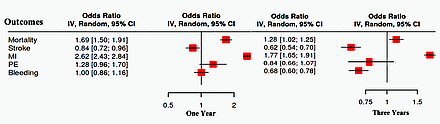
Results: At 1 year, OAC monotherapy had higher mortality (10.8% vs. 6.7%; OR 1.690, CI [1.497,1.907], p<0.001), lower stroke risk (5.4% vs. 6.4%; OR 0.835, CI [0.725,0.963], p=0.013), higher MI (36.2% vs. 17.8%; OR 2.624, CI [2.426,2.839], p<0.001), with no difference in PE (1.6% vs. 1.3%; OR 1.2, CI [0.965,1.699], p=0.086) or bleeding (5.3% each; OR 1.0, CI [0.862,1.161], p=1.0). At 3 years, OAC monotherapy demonstrated sustained higher mortality (13.6% vs. 12.3%; OR 1.128, CI [1.021,1.245], p=0.018), higher MI (36.7% vs. 24.6%; OR 1.772, CI [1.647,1.907], p<0.001), reduced stroke risk (5.8% vs. 9.1%; OR 0.617, CI [0.542,0.702], p<0.001), and lower bleeding (6.0% vs. 8.5%; OR 0.683, CI [0.600,0.778], p<0.001), with no difference in PE.
Conclusions: In this large, real-world matched cohort, OAC monotherapy in patients with AF and stable CAD post-PCI was associated with increased mortality and significantly higher myocardial infarction rates despite a reduction in ischemic stroke compared to combined therapy. OAC monotherapy was associated with significantly lower bleeding risk at 3 years.
Mestarihi, Aseed
(
University of central Florida
, Gainesville , Florida , United States )
Obeidat, Omar
(
UCF HCA North Florida
, Gainesville , Florida , United States )
Alqudah, Qusai
(
UCF-North Florida Hospital
, Gainesville , Florida , United States )
Rayyan, Abdallah
(
University of Central Florida
, Gainesville , Florida , United States )
Mansour, Mohamad
(
MedStar Health
, Baltimore , Maryland , United States )
Daise, Mohd
(
University of Central Florida
, Gainesville , Florida , United States )
Kc, Anil
(
University of Central Florida
, Gainesville , Florida , United States )
Author Disclosures:
Aseed Mestarihi:DO NOT have relevant financial relationships
| Omar Obeidat:DO NOT have relevant financial relationships
| Qusai Alqudah:DO NOT have relevant financial relationships
| Abdallah Rayyan:DO NOT have relevant financial relationships
| Mohamad Mansour:DO NOT have relevant financial relationships
| Mohd Daise:DO NOT have relevant financial relationships
| ANIL KC:DO NOT have relevant financial relationships