The Starved Heart: Pericarditis in Extreme Anorexia Nervosa
Abstract Body (Do not enter title and authors here): Background: Anorexia nervosa (AN) is a psychiatric disorder defined by restrictive eating, fear of weight gain, and distorted body image, with a lifetime prevalence of ~4% among females. In its severe form, AN leads to multi-organ complications, particularly affecting the cardiovascular system. Bradycardia, hypotension, and asymptomatic pericardial effusions occur in up to 25% of patients. However, symptomatic pericarditis in AN has not been previously documented.
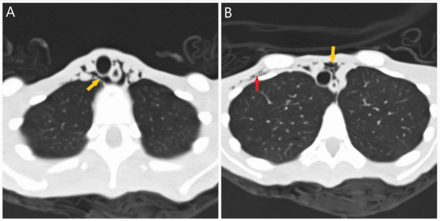
Case Presentation: A 21-year-old female with depression presented with two days of sharp, positional chest pain, dyspnea, palpitations, and weakness. She reported eating less than one meal per day, running 22 miles daily, self-induced vomiting, and experiencing one year of amenorrhea. On exam, her BMI was 10.7 kg/m^2, with lanugo, proximal muscle weakness, and a pericardial friction rub. Labs showed hypokalemia, hypophosphatemia, transaminitis, elevated CK, and leukocytosis. ECG demonstrated diffuse ST elevations and PR depression in aVR. Transthoracic echocardiography revealed a moderate pericardial effusion without tamponade (Figure 1). CT chest showed pneumomediastinum and subcutaneous emphysema without evidence of esophageal perforation (Figure 2). Workup for infectious, autoimmune, ischemic, and thyroid causes was negative. She was diagnosed with severe AN and major depressive disorder. Management included IV fluids, electrolyte repletion, and nutritional support. Pericarditis was treated with ibuprofen and colchicine. Psychiatric therapy included olanzapine and mirtazapine for appetite stimulation and mood support. She was discharged to a structured inpatient nutritional rehabilitation program.
Discussion: This is the first reported case of symptomatic pericarditis in AN. While pericardial effusions are often asymptomatic and linked to myocardial and pericardial fat loss, this case suggests purging-induced esophageal microperforations may cause subclinical mediastinitis, triggering pericardial inflammation. Cardiovascular complications occur in up to 87% of patients with AN. A high index of suspicion for pericarditis is warranted in malnourished patients presenting with chest pain. ECG, echocardiography, and imaging are essential.
Conclusion: Symptomatic pericarditis is a rare but serious cardiac complication of AN. Early diagnosis and coordinated multidisciplinary care are essential for recovery.
Mansour, Mohamad
(
MedStar Georgetown University
, Baltimore , Maryland , United States )
Haque, Obaid
(
MedStar Georgetown University
, Baltimore , Maryland , United States )
Mestarihi, Aseed
(
University of central Florida
, Gainesville , Florida , United States )
Author Disclosures:
Mohamad Mansour:DO NOT have relevant financial relationships
| Obaid Haque:DO NOT have relevant financial relationships
| Aseed Mestarihi:DO NOT have relevant financial relationships