Mortality risk and procedural complications with general anesthesia compared to monitored anesthesia care in percutaneous LAAo: A Propensity-Matched Real-World Analysis
Abstract Body (Do not enter title and authors here): Introduction: During percutaneous LAAo, intraprocedural guidance with TEE and fluoroscopy is the standard of care. While general anesthesia with intubation (GA) has historically been the primary choice, the use of monitored anesthesia care (MAC) and conscious sedation is rising. The comparative impact of general anesthesia with intubation (GA) on clinical outcomes remains uncertain. We sought to evaluate the risk of adverse clinical outcomes and mortality compared to MAC.
Methods Using the TriNetX US Collaborative Network, we conducted a retrospective propensity-matched cohort study of patients undergoing LAAo from January 2015 to May 2025. GA was defined using ICD-10-PCS codes for endotracheal intubation or mechanical ventilation within ±1 day of LAAo. Outcomes were assessed within 1 year post-index using risk difference (RD), risk ratio (RR), hazard ratio (HR), and log-rank p-values. Propensity score matching (1:1) was applied.
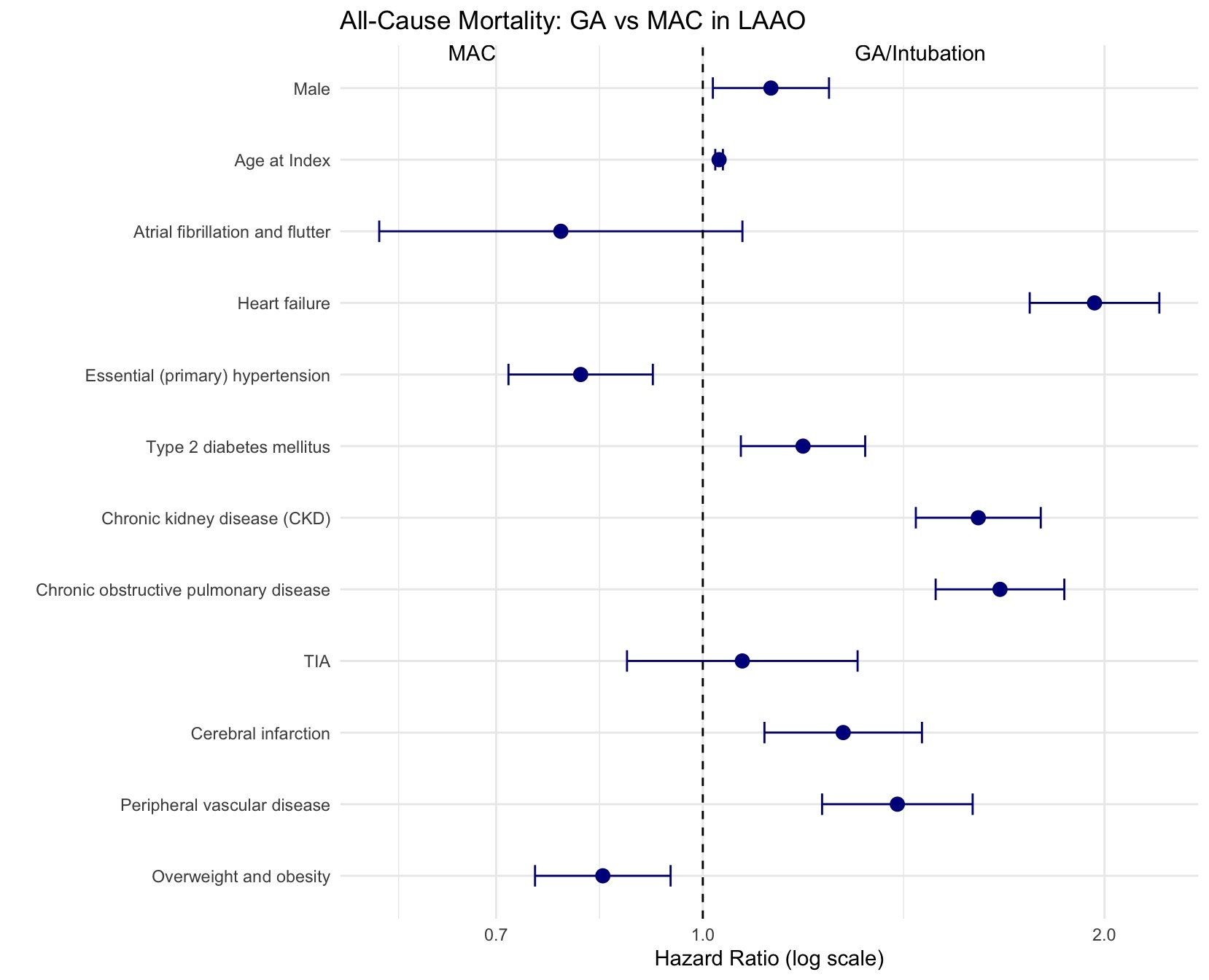
Results Two comparable cohorts (n = 160) were generated after propensity matching. The mean age was 76.6 years, 44% were female, and 74% were White in both cohorts. GA was associated with significantly higher all-cause mortality (RR 3.40 [1.74–6.65]; HR 5.51 [2.44–12.44], p<0.001), respiratory failure (RR 4.46 [2.55–7.81]; HR 5.84 [3.20–10.68], p<0.001), pericardial effusion (RR 2.70 [1.35–5.39]; HR 3.97 [1.80–8.75], p<0.001), and device embolization (6.3% vs 0.0%; RD +6.3% [2.5–10.0], p=0.001). Rates of ischemic stroke, hemorrhagic stroke, vascular complications, cardiac tamponade, and in-hospital mortality were similar between groups (all p>0.05). A forest plot displaying the adjusted HR’s for all the covariates included in the Cox proportional hazards model evaluating all-cause mortality in LAAO patients is shown in image-1.
Conclusion Based on prior literature MAC utilization of percutaneous LAAo is increasing. While studies show that MAC is feasible during LAAo, general anesthesia use is still predominant. We find that there is a significant increase in all-cause mortality, respiratory failure, pericardial effusion, and device embolization despite GA use. Complete airway control, patient immobilization facilitating accurate transeptal puncture, complex left atrial appendage anatomy, and institutional expertise all factor into the ultimate decision of MAC vs GA. Our findings support the preferential use of MAC in suitable patients and emphasize the need for careful perioperative planning.
Khan, Zainab Zaib
(
Metrohealth Medical Center
, Cleveland , Ohio , United States )
Shehzad, Mustafa
(
Hackensack University Medical Center
, Hackensack , New Jersey , United States )
Sajid, Ahmed
(
PIMS, islamabad
, Islamabad , Pakistan )
Khan, Farva Zaib
(
Metrohealth Medical Center
, Cleveland , Ohio , United States )
Shehzad, Dawood
(
University of South Dakota
, Sioux Falls , South Dakota , United States )
Anwar, Muhammad Zahid
(
Lady Reading Hospital, Peshawar
, Peshawar , Pakistan )
Chaudhry, Hammad
(
University of South Dakota
, Sioux Falls , South Dakota , United States )
Ahmed, Mamoon
(
University of South Dakota
, Sioux Falls , South Dakota , United States )
Rajpurohit, Naveen
(
University of South Dakota
, Sioux Falls , South Dakota , United States )
Author Disclosures:
Zainab Zaib Khan:DO NOT have relevant financial relationships
| Rafia Irfan Waheed:DO NOT have relevant financial relationships
| Sunia Shabir chaudhary:No Answer
| Hammad Chaudhry:DO NOT have relevant financial relationships
| Mamoon Ahmed:No Answer
| Naveen Rajpurohit:DO NOT have relevant financial relationships
| Mustafa Shehzad:DO NOT have relevant financial relationships
| Ahmed Sajid:DO NOT have relevant financial relationships
| Farva Zaib Khan:No Answer
| Dawood Shehzad:DO NOT have relevant financial relationships
| Muhammad Zahid Anwar:DO NOT have relevant financial relationships
| Wassey Abdul:No Answer
| Aoun Zaib Khan:DO NOT have relevant financial relationships
| Dawlat Khan:No Answer