Outcomes of patients with Cardiac Sarcoidosis (CS) implanted with an implantable cardiac defibrillator (ICD).
Abstract Body (Do not enter title and authors here): Background: We aimed to evaluate the outcomes of patients with confirmed and possible cardiac sarcoidosis who had an ICD implant and identify predictors of ventricular arrhythmias and mortality in this patient population.
Methods: We performed a retrospective study patients with a diagnosis of cardiac sarcoidosis (CS) at Mayo Clinic and had an ICD implanted for primary or secondary prevention indication. Adult patients (≥18 years) with a diagnosis of possible or confirmed (biopsy-proven) CS with an ICD implanted between 1993 and 2022 were included. Primary outcomes included sustained ventricular arrhythmia (VT) resulting in a documented appropriate ICD shock and death from any cause. Secondary outcomes included ICD-related complications.
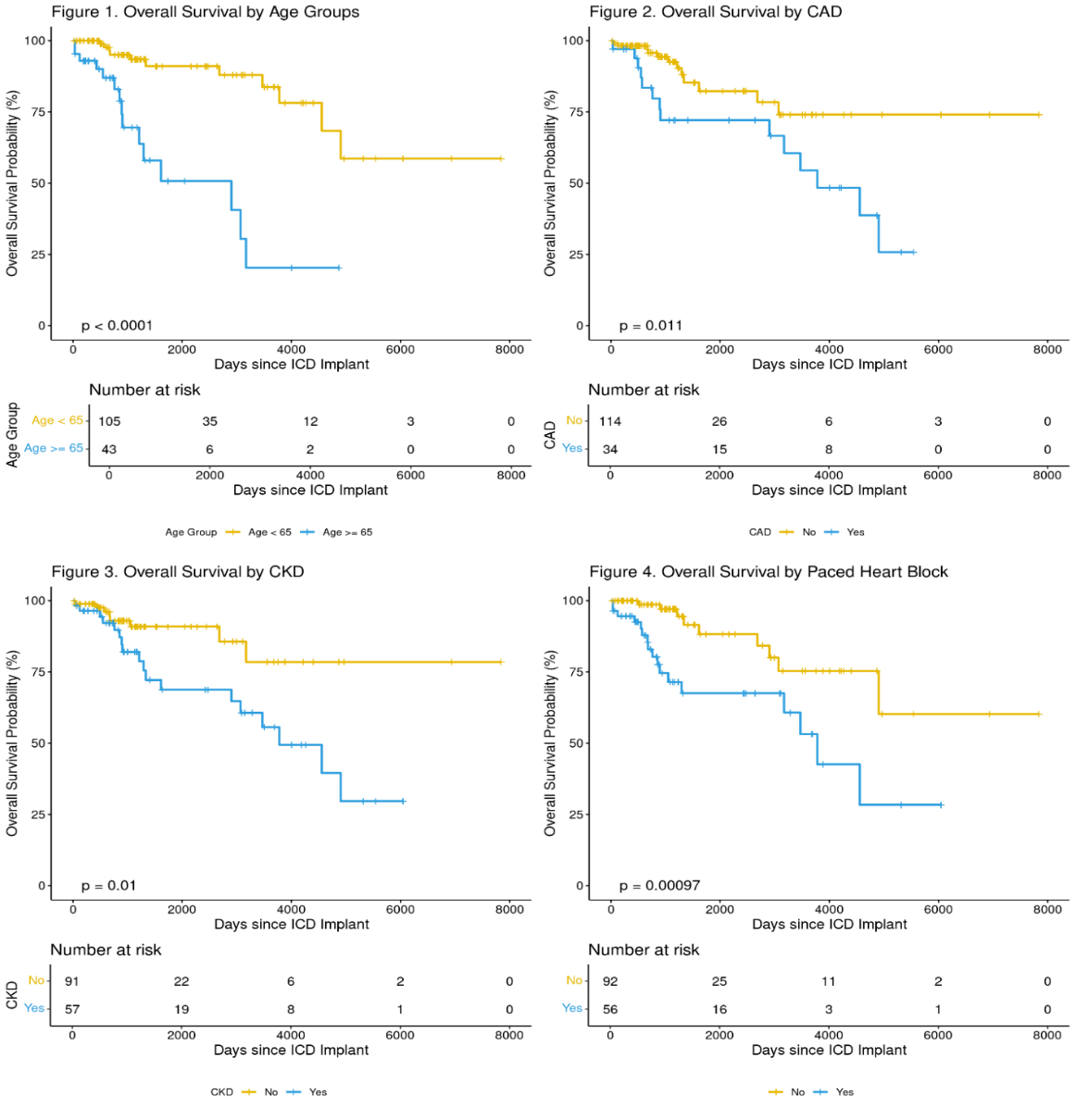
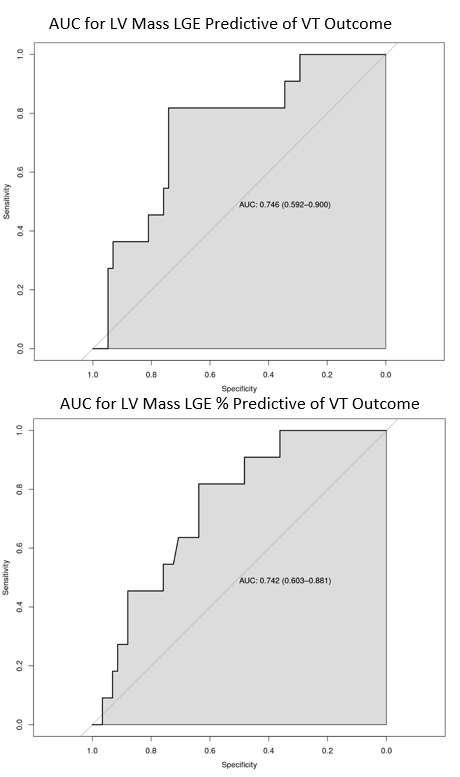
Results: We identified 148 patients, in which 23 patients (15.5%) experienced VT events with a total of 160 treated episodes. 4 patients (2.7%) experienced inappropriate ICD shocks (11 episodes). During a median follow up of 3.1 years, 26 patients deceased, and the overall survival was 98% and 77% at 1 and 5 year. Older age, CAD, CKD, paced rhythm and QRS duration were associated with worse survival (Figure 1 – 4). Device related complications were rare, except for the higher percentage of CHF in patients with VT after implant, however this was not statistically significant. Patients with ICD therapies were younger (53 vs 58 years, p=0.029), had higher LGE burden (26.9 vs 16.3%, p=0.01), and higher percentage of LV mass (26.9 vs 16.3, p=0.011). Multivariate logistic regression model which showed that patients with biopsy proven sarcoidosis had significantly higher odds of VT events (OR: 3.04, 95% CI: 1.02 to 9.08, p = 0.046). In patients with increased LV mass (every 10 g increase), the odds of developing VT increased by 1.49 (95% CI: 1.02 to 2.19, p = 0.041). LV mass and LGE percentage showed fair ability of predicting the outcome by ROC analysis. Youden’s index showed 26 for LV mass and 16% for LGE percent as the optimal cut-off points for predicting VT outcomes (Figure 5). The sensitivity, specificity, positive predictive value, negative predictive value were 81.8%, 74.1%, 37.5%, 95.6% and 75.4% respectively for an LV mass of 26 grams and 81.8%, 63.8%, 30.0%, 94.9% and 66.7% respectively for an LGE percentage of 16%. Conclusion: LGE burden continues to be a major predictor for VT events in patients with CS. Myocardial tissue burden and electrical abnormalities from CS predict mortality than myocardial function loss.
Arunachalam Karikalan, Suganya
(
Christus health
, Longview , Texas , United States )
Yusuf, Ali
(
Texas tech university health sciences center Internal medicine residency program
, Amarillo , Texas , United States )
Cheema, Kamal
(
Mayo Clinic Arizona
, Scottsdale , Arizona , United States )
Zhang, Nan
(
Mayo Clinic Arizona
, Scottsdale , Arizona , United States )
El Masry, Hicham
(
Mayo CLinic AZ
, Phoenix , Arizona , United States )
Author Disclosures:
Suganya Arunachalam Karikalan:DO NOT have relevant financial relationships
| Ali Yusuf:DO NOT have relevant financial relationships
| Kamal Cheema:No Answer
| Nan Zhang:DO NOT have relevant financial relationships
| Hicham El Masry:No Answer
Syed Alveena, Motairek Issam, El Hajjar Abdel Hadi, Abdulhai Farah, Saraswati Ushasi, Safdar Ahmad, Bhalla Jaideep Singh, Wang Tom Kai Ming, Ramchand Jay, Klein Allan