Antithrombotic Strategy and Long-term Outcome In dialysis patients with coexisting acute coronary syndrome and atrial fibrillation: a nationwide study
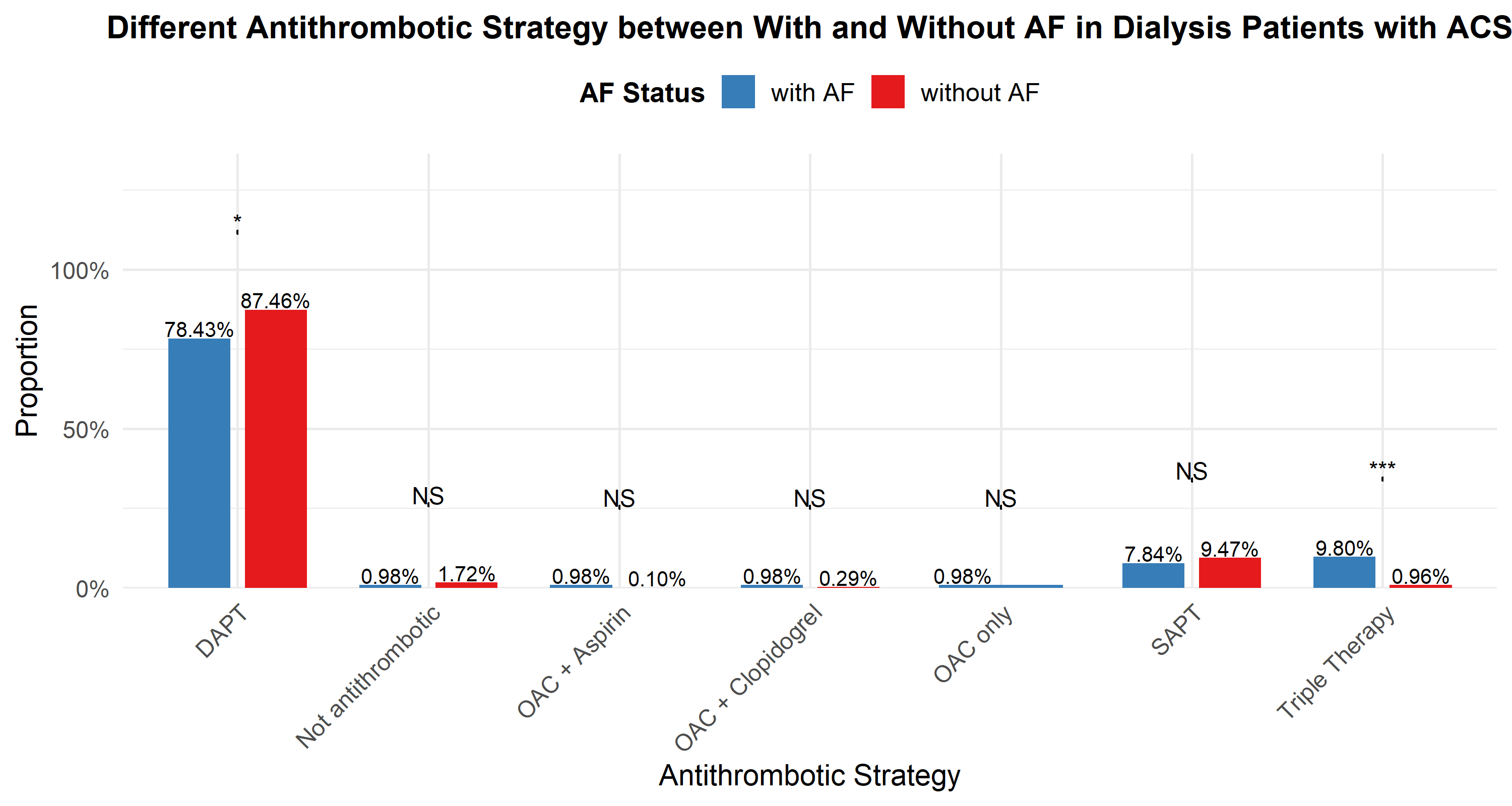
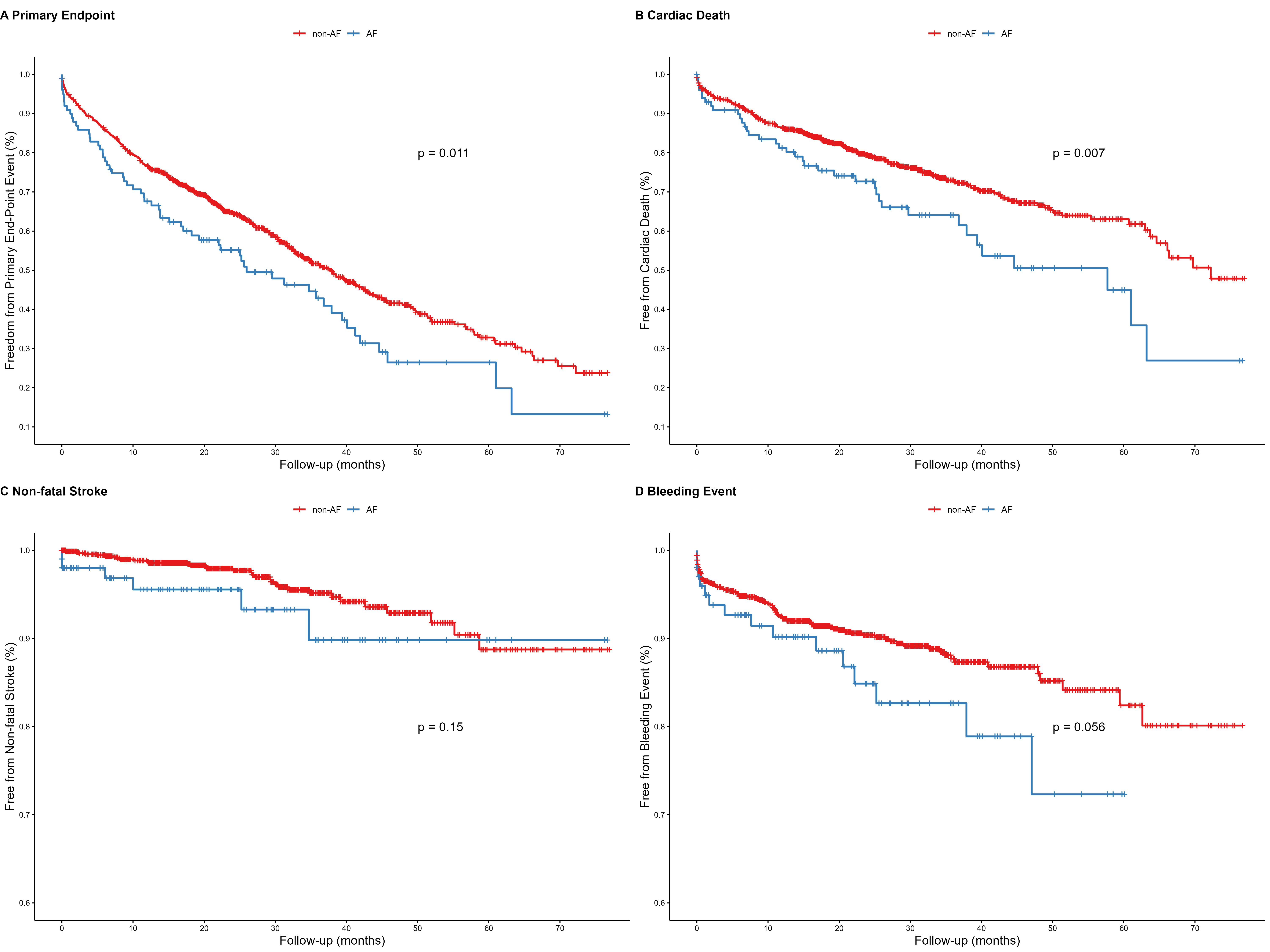
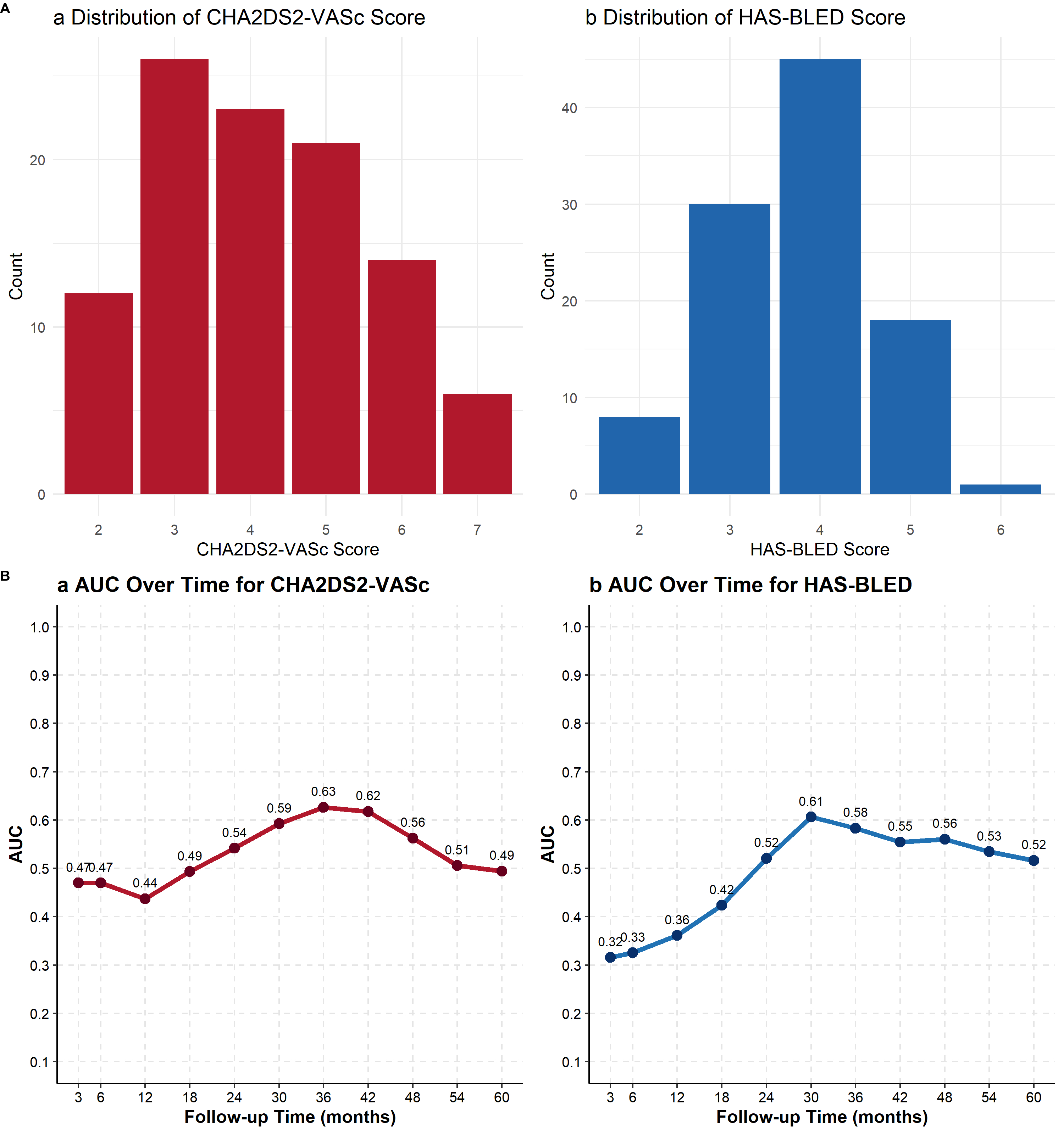
Abstract Body (Do not enter title and authors here): Background: Dialysis patients with both acute coronary syndrome (ACS) and atrial fibrillation (AF) face high thrombotic and bleeding risks. The optimal antithrombotic strategy and long-term outcomes remain unclear. Methods: We analyzed data from the CRUISE-R, a nationwide, multicenter, retrospective cohort in China. Patients were grouped by AF status. The primary endpoint was a composite of all-cause mortality, non-fatal myocardial infarction, and stroke. Baseline features, antithrombotic strategies, and outcomes were compared. betwee groups. Results: Among 1,147 patients, 102 (8.9%) had AF. Compared to those without AF, AF patients were older (65.1 vs. 61.4 years, p < 0.001), had higher proBNP (30,826 vs. 21,153 pg/ml, p = 0.015), and larger left atrial diameter (43.6 vs. 40.9 mm, p = 0.001). Triple therapy (OAC + aspirin + clopidogrel) was more common in AF patients (9.8% vs. 0.96%, p < 0.001) (Figure 1). Over 22.9 months of follow-up, 511 patients (44.6%) reached the primary endpoint—450 (43.1%) without AF vs. 61 (59.8%) with AF. AF patients had higher composite event and cardiac mortality rates (p < 0.05), but stroke and bleeding rates were not significantly different (p = 0.18 and 0.056, respectively) (Figure 2). Cox regression analysis identified AF as an independent predictor of the primary endpoint (HR 1.46, 95% CI: 1.07–1.98, p = 0.016) and cardiac death (HR 1.52, 95% CI: 1.02–2.27, p = 0.038). Triple antithrombotic therapy was independently associated with an increased risk of bleeding (HR 5.88, 95% CI: 1.41–24.52, p = 0.015). Among the 106 patients with both ACS and AF, mean CHA2DS2-VASc and HAS-BLED scores were 3.8 and 3.4 (Figure 3A). However,both scores demonstrated limited predictive value for non-fatal stroke and bleeding events in this population, with area under the curve (AUC) values below 0.65 (Figure 3B). Conclusion: In dialysis patients with ACS, the presence of atrial fibrillation is associated with a significantly worse prognosis, including higher primary composite endpoint and cardiac mortality, although the incidence of stroke is not significantly increased. Triple antithrombotic therapy markedly raises the risk of bleeding and should be used with caution. Standard risk scores such as CHA2DS2-VASc and HAS-BLED have limited predictive power in this population. Further research is needed to develop more effective risk stratification tools for identifying high-risk subgroups prone to thrombotic and bleeding events.
An, Shuoyan
(
China-Japan Friendship Hospital
, Beijing , China )