Association Between Pre-Operative History of Significant Bleeding and Post-Operative Cardiovascular Events Following Lower Extremity Revascularization
Abstract Body (Do not enter title and authors here): Background and Hypothesis: Patients with symptomatic peripheral artery disease (PAD) frequently undergo lower extremity revascularization (LER) but remain at increased risk of major adverse cardiovascular and limb events following the procedure. Patients with a bleeding history tend to have lower platelet activity and thus may be at lower risk for a cardiovascular event following LER.
Methods/Approach: Patients aged ≥21 years and scheduled for non-emergent LER were recruited for participation. Based on self-reported history of seven types of significant bleeding (significant nosebleeds, hematuria, gastrointestinal bleeding, oral cavity bleeding, bleeding after surgery or major trauma, and non-trauma related central nervous system or ocular bleeding), 289 participants with complete information were stratified into three groups: no history of significant bleeding (186, 64%), history of significant bleeding not requiring medical attention (48, 17%), and history of significant bleeding requiring medical attention (55, 19%).
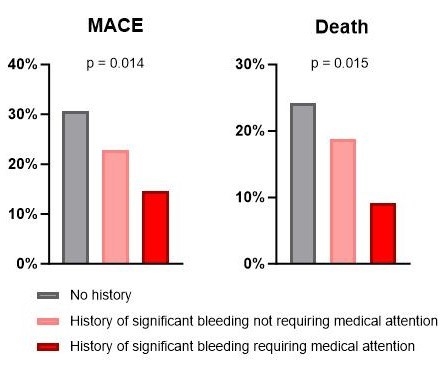
Results: There were no differences between groups observed in age, sex, race, ethnicity, diabetes, hypertension and prior coronary artery disease. Body mass index was lowest in the no-history group, higher in the non-medical-attention group, and highest in the medical-attention group (26.2, 27.8, 28.1 kg/m2, respectively; p=0.012). After a median follow-up of 18 months, a composite of major adverse cardiovascular events (MACE; death, myocardial infarction, and stroke) and death occurred in 26.3% and 20.4% of all participants, respectively. History of bleeding was associated with improved clinical outcomes, with MACE and death occurring less frequently in the non-medical-attention group and less frequently still in the medical-attention group. MACE occurred in 30.6%, 22.9%, and 14.5% of participants in the no-history, non-medical-attention, and medical-attention groups, respectively (Figure 1, p = 0.014). Death occurred in 24.2%, 18.8%, and 9.1% of participants in the no-history, non-medical-attention, and medical-attention groups, respectively (Figure 1, p = 0.015).
Conclusion: Pre-operative history of bleeding exhibits a relationship with adverse outcomes following LER. Participants with a history of significant bleeding, especially significant bleeding requiring medical attention, experience lower risk of MACE and death.
Bresnahan, David
(
NYU Langone Health
, New York , New York , United States )
Xia, Yuhe
(
NYU Langone Health
, New York , New York , United States )
Luttrell-williams, Elliot
(
NYU Langone Health
, New York , New York , United States )
Murphy, Lila
(
NYU Langone Health
, New York , New York , United States )
Berger, Jeffrey
(
NYU Langone Health
, New York , New York , United States )
Author Disclosures:
David Bresnahan:DO NOT have relevant financial relationships
| Yuhe Xia:DO NOT have relevant financial relationships
| Elliot Luttrell-Williams:DO NOT have relevant financial relationships
| Lila Murphy:DO NOT have relevant financial relationships
| Jeffrey Berger:No Answer