Systematic Review and Meta-Analysis on CardioMEMS for Enhanced Heart Failure Management: Examining Randomized Controlled Trials and Observational Studies
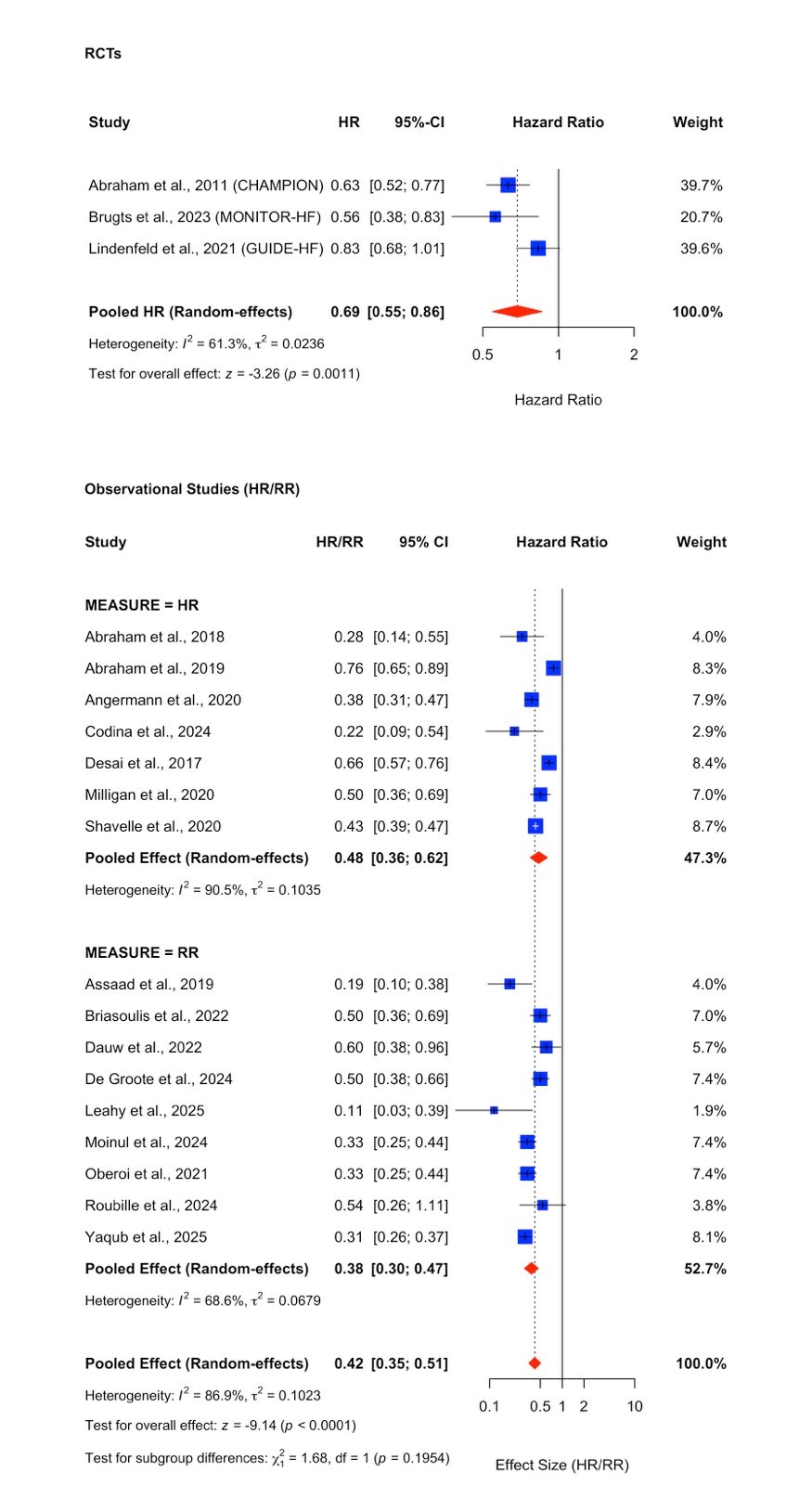
Abstract Body (Do not enter title and authors here): Introduction Patients with severe or advanced heart failure symptoms are often hospitalized for acute decompensated heart failure despite being on guideline-directed medical therapies (GDMT). Some randomized control trials have shown that implanting CardioMEMS, a pressure sensor device placed inside the pulmonary artery to measure systolic and diastolic pulmonary pressure, can improve rates of heart failure hospitalization without affecting mortality. However, many non-randomized observational studies have not been thoroughly investigated and compared with the findings from RCTs. Objectives Compare the one-year heart failure hospitalization rates, cardiovascular mortality, and all-cause mortality between patients with and without CardioMEMS. Methods A systematic search of PubMed, Scopus, Embase, Cochrane Library, and Web of Science was conducted through April 30, 2025. A total of 420 studies, including randomized control trials, prospective single-arm studies, retrospective cohorts, and case-control studies, were screened. Studies that reported a Hazard ratio (HR) or relative risk (RR) were included. Random effects models were utilized to derive pooled HR and RR. Study quality and bias were evaluated using the Newcastle-Ottawa scale, funnel plots, and Egger’s test. Results A total of 19 studies, three RCTs and 16 observational studies, with 11,343 participants, were included. The data showed a mean age ranging from 60.9 to 75.5 years, 34.5% women, 76.1-83.7% Whites, and 12.6-18.4% Blacks. 65.3% had HFrEF, mostly NYHA class III. Pooled RCTs showed a 31% relative risk reduction (HR: 0.69; 95% CI: 0.55–0.86; I2 = 61.3%). Observational studies also showed benefit: those reporting hazard ratios had a pooled HR of 0.48 (95% CI: 0.36–0.62; I2 = 90.5%), while those reporting risk ratios yielded a pooled RR of 0.38 (95% CI: 0.30–0.47; I2 = 68.7%). All-cause mortality from RCTs showed no difference (HR: 0.97, CI: 0.74-1.28). However, the observational studies lacked sufficient data on cardiovascular and all-cause mortality.
Conclusion
CardioMEMS implantation was associated with a significant reduction in one-year heart failure hospitalizations across study designs. Both randomized and observational studies reported comparable outcomes in controlled and real-world settings.
Weldehana, Amha
(
Westchester Medical Center
, Valhalla , New York , United States )
Tessema, Abel
(
University of Manchester
, Manchester , United Kingdom )
Fentie, Meseker
(
Drexel University
, Philadelphia , Pennsylvania , United States )
Yeneneh, Beeletsega
(
University of Arizona
, Phoenix , Arizona , United States )
Siraw, Bekure
(
Ascension Saint Joseph - Chicago
, Chicago , Illinois , United States )
Fuisz, Anthon
(
Westchester Medical Center
, Valhalla , New York , United States )
Author Disclosures:
Amha Weldehana:DO NOT have relevant financial relationships
| Abel Tessema:No Answer
| Meseker Fentie:DO NOT have relevant financial relationships
| Samrawit Zewde:DO NOT have relevant financial relationships
| Beeletsega Yeneneh:DO NOT have relevant financial relationships
| Bekure Siraw:DO NOT have relevant financial relationships
| Anthon Fuisz:No Answer