Higher Blood Pressure Time-in-Target Range May Improve Primary Cardiovascular Outcome in Patients with Hypertension and Coronary Artery Disease
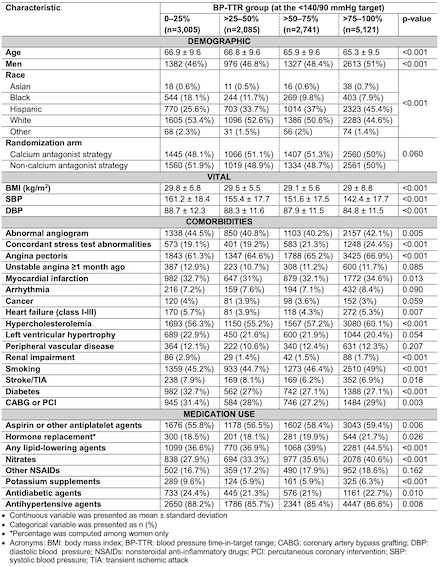
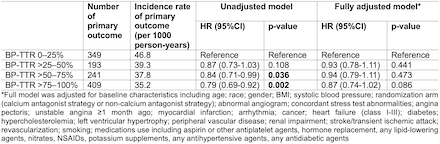
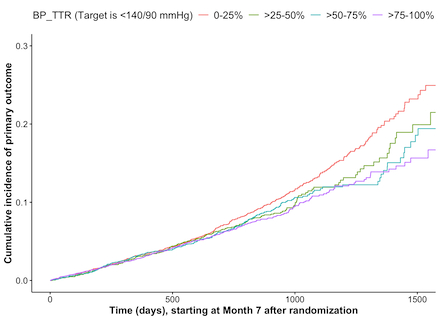
Abstract Body (Do not enter title and authors here): Introduction: Higher blood pressure Time-in-Target Range (BP-TTR) has been associated with lower risk of cardiovascular outcomes. However, the prognostic value of BP-TTR among patients with hypertension (HTN) and coronary artery disease (CAD) remains unclear. Research Question: Is higher BP-TTR over a 6-month period associated with a reduced risk of primary cardiovascular outcome (composite all-cause mortality, nonfatal myocardial infarction, nonfatal stroke) among patients with HTN+CAD? Methods: In this post-hoc analysis of the randomized INternational VErapamil-trandolapril STudy (INVEST), we pooled patients (aged ≥50 years with HTN+CAD) randomized to a calcium antagonist or non-calcium antagonist strategy, which had equivalent outcomes in INVEST. Of 22,576 INVEST participants, we identified those with ≥4 BP readings, and without the primary outcome or loss to follow-up within the first 6 months post-randomization (including randomization date). We performed linear interpolation with constant extrapolation using eligible participants’ BP readings during this 6-month period (168 days) to estimate BP-TTR, defined as the proportion of days with BP readings below the target (140/90 mmHg) over the 168-day window. Cox proportional hazards regression was used to examine the association between BP-TTR in the first 6 months post-randomization and the primary outcome thereafter. Results: A total of 12,952 eligible participants were included (mean±SD age, 66.1±9.6 years; 48.6% men). Among four BP-TTR groups (0–25%, >25–50%, >50–75%, and >75–100%), individuals with a BP-TTR of >75–100% had the lowest incidence rate of the primary outcome (35.2 per 1,000 person-years). Compared to individuals in the lowest BP-TTR group, those in higher BP-TTR groups had a reduced risk of the primary outcome in both unadjusted and adjusted models. However, statistically significant reductions were observed only in the unadjusted model for the BP-TTR >50–75% group (hazard ratio [95% CI], 0.84 [0.71-0.99]; p=0.036), and the BP-TTR >75–100% group (0.79 [0.69-0.92]; p=0.002). Conclusions: In patients with HTN+CAD, higher BP-TTR at the target of <140/90 mmHg may be associated with a reduced risk of the composite outcome of all-cause mortality, nonfatal myocardial infarction, and nonfatal stroke, though statistical significance was not reached after adjustment. As a next step, we plan to conduct additional analyses applying alternative BP targets and assessing other outcomes in the INVEST.
Nguyen, Ngoc Thuy Tram
(
University of Florida
, Gainesville , Florida , United States )
Pepine, Carl
(
University of Florida
, Gainesville , Florida , United States )
Smith, Steven
(
University of Florida
, Gainesville , Florida , United States )
Author Disclosures:
Ngoc Thuy Tram Nguyen:DO NOT have relevant financial relationships
| Carl Pepine:No Answer
| Steven Smith:DO NOT have relevant financial relationships