Temporal Trends in Major Adverse Cardiovascular Events Following Hospitalization for Myocardial Infarction Between 2008-2022: Insights from the Veterans Affairs Healthcare System
Abstract Body (Do not enter title and authors here): Background: Over 800,000 individuals are hospitalized for a myocardial infarction (MI) annually in the United States. Temporal trends in post-discharge outcomes are uncertain.
Question: Among Veterans who survive an MI hospitalization, how have post-discharge outcomes changed?
Methods: Veterans who survived an MI hospitalization within or outside the VHA between 2008-2022 were identified based on a principal diagnosis of MI from an acute care hospitalization. We identified comorbidities, vital signs, and laboratory values pre-hospitalization. The primary outcome was a 4-point composite MACE (death, MI, ischemic stroke, and heart failure (HF) hospitalization) over 1 year post-discharge. Temporal trends were analyzed by comparing outcomes across 3 time periods (2008-2012, 2013-2017, and 2018-2022) with the Cuzick rank test. We also evaluated 1-year death alone and performed a landmark analysis evaluating 1-year death following HF hospitalization within the first 12 months post-MI. The annual change in outcomes was examined while adjusting for demographics, comorbidities, pre-admission vital signs and laboratory values, and STEMI vs. NSTEMI classification.
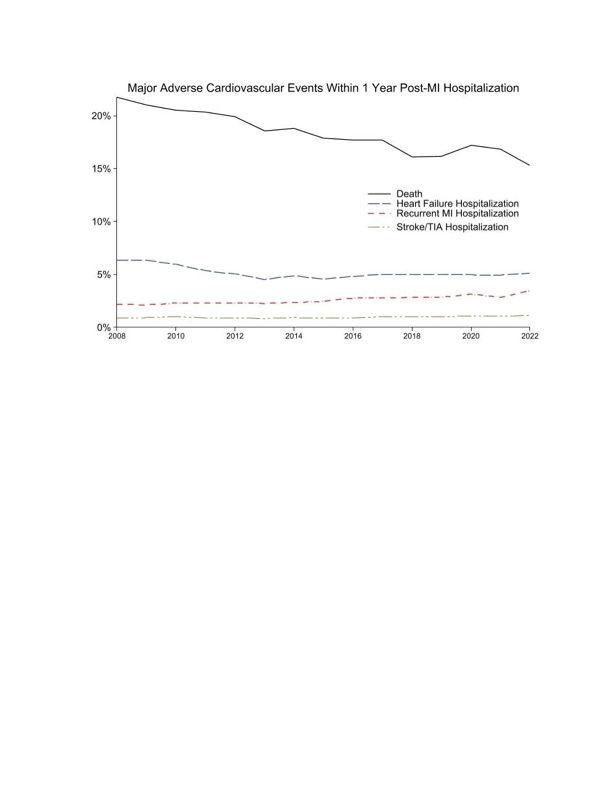
Results: There were 444,659 Veterans with a non-fatal MI hospitalization between 2008 and 2022. The median age was 73 (interquartile range: 66-80) and 1.8% were women. Over time, the proportion with STEMI decreased (2008-2012: 26.1%, 2013-2017: 23.1%, and 2018-2022: 23.1%; p<0.01). The proportion with inpatient revascularization decreased from 49.6% to 48.1% to 36.9% (p<0.01). The 1-year risk of the composite MACE outcome decreased from 26.1% to 23.2% to 22.2% (p<0.01) across time periods. After adjustment, there was a 3.9% annual relative decrease in the odds of 1-year MACE (OR: 0.965; 95% CI: 0.963-0.967). The risk of 1-year death post-MI hospitalization decreased from 20.7% to 18.1% to 16.3% (p<0.01) (Figure). After adjustment, there was a 4.2% annual relative decrease in the odds of 1-year mortality (OR 0.958 per year; 95% CI: 0.956-0.960). There were 23,048 (5.2%) Veterans with HF hospitalization within 12 months of MI discharge. Among this cohort, 44.9% died within 1-year post-HF hospitalization.
Conclusion: Among Veterans, the risk of death post-MI hospitalization has improved over time. However, over 1 in 5 Veterans post-MI continue to have major adverse cardiovascular outcomes within 1 year. Veterans with a HF hospitalization post-MI are at substantially elevated risk of death.
Sandhu, Alexander
(
Stanford University, VAPAHCS
, Palo Alto , California , United States )
Furst, Adam
(
Stanford University, VAPAHCS
, Palo Alto , California , United States )
Rodriguez, Fatima
(
STANFORD UNIVERSITY
, Palo Alto , California , United States )
Kalwani, Neil
(
Stanford University, VAPAHCS
, Palo Alto , California , United States )
Maron, David
(
Stanford University
, Millbrae , California , United States )
Nallamshetty, Shriram
(
Stanford University, VAPAHCS
, Palo Alto , California , United States )
Din, Natasha
(
Stanford University, VAPAHCS
, Palo Alto , California , United States )
Fan, Michael
(
Novo Nordisk
, Los Angeles , California , United States )
Khachatourian, Kat
(
Novo Nordisk
, Plainsboro , New Jersey , United States )
Skaar, Jeffrey
(
Novo Nordisk
, Plainsboro , New Jersey , United States )
Tonnu-mihara, Ivy
(
Novo Nordisk Inc.
, Huntington Beach , California , United States )
Author Disclosures:
Alexander Sandhu:DO have relevant financial relationships
;
Consultant:Reprieve Cardiovascular:Active (exists now)
; Consultant:Clearly:Active (exists now)
; Research Funding (PI or named investigator):NOVO NORDISK:Active (exists now)
; Research Funding (PI or named investigator):Novartis:Active (exists now)
; Research Funding (PI or named investigator):Bayer:Active (exists now)
; Research Funding (PI or named investigator):Astra Zeneca:Active (exists now)
| Jeffrey Skaar:DO have relevant financial relationships
;
Employee:Novo Nordisk:Active (exists now)
; Individual Stocks/Stock Options:Trinity Life Sciences:Active (exists now)
; Individual Stocks/Stock Options:Novo Nordisk:Active (exists now)
| Ivy Tonnu-Mihara:DO have relevant financial relationships
;
Employee:NNI:Active (exists now)
| Adam Furst:DO NOT have relevant financial relationships
| Fatima Rodriguez:DO have relevant financial relationships
;
Consultant:HealthPals:Past (completed)
; Consultant:Cleerly Health:Active (exists now)
; Consultant:Amgen:Active (exists now)
; Consultant:iRhythm:Active (exists now)
; Consultant:HeartFlow:Active (exists now)
; Consultant:Arrowhead Pharmaceuticals:Active (exists now)
; Consultant:Edwards:Active (exists now)
; Consultant:Inclusive Health:Active (exists now)
; Consultant:Esperion Therapeutics:Past (completed)
; Consultant:Kento Health:Active (exists now)
; Consultant:Movano Health:Active (exists now)
; Consultant:NovoNordisk:Past (completed)
; Consultant:Novartis:Active (exists now)
| Neil Kalwani:DO NOT have relevant financial relationshipsShriram Nallamshetty:No Answer
| Natasha Din:DO NOT have relevant financial relationships
| Michael Fan:DO have relevant financial relationships
;
Employee:Novo Nordisk:Active (exists now)
; Individual Stocks/Stock Options:Novo Nordisk:Active (exists now)
| Kat Khachatourian:DO have relevant financial relationships
;
Employee:Novo Nordisk:Active (exists now)
; Individual Stocks/Stock Options:Novo Nordisk:Active (exists now)