Clinical Outcomes Among Individuals with Persistent Systemic Inflammation Following Myocardial Infarction: Insights from the Veterans Affairs Healthcare System
Abstract Body (Do not enter title and authors here):
Introduction Acute myocardial infarction (MI) triggers acute inflammation. A subset of patients experience subsequent chronic systemic inflammation (SI) post-MI.
Question Among patients with a prior MI, is SI associated with a higher risk of major adverse cardiovascular (CV) events?
Methods We identified Veterans with a nonfatal MI from 2008-2022 and a subsequent outpatient high-sensitivity C-reactive protein (hsCRP) measurement 60-730 days post-MI. Veterans with select comorbidities known to increase SI and mortality (e.g., active cancer or end-stage renal or severe hepatic diseases) were excluded.
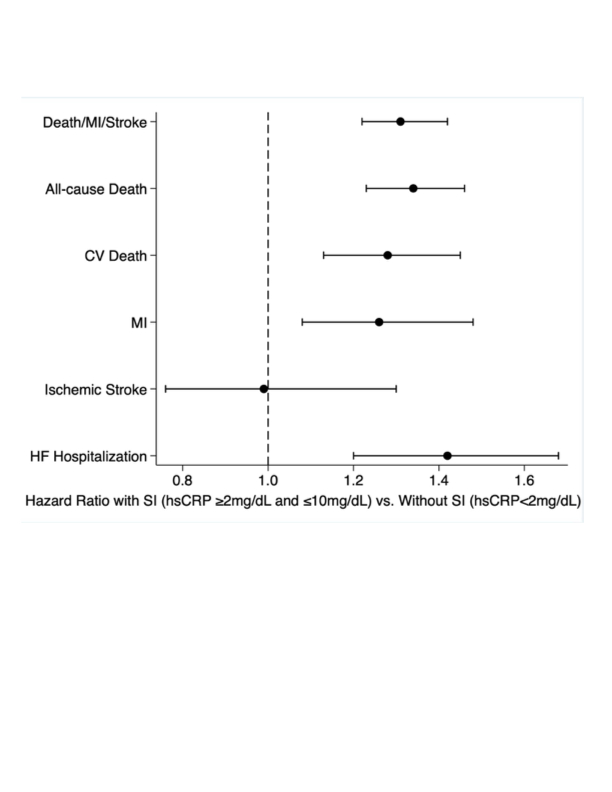
The primary outcome was a composite of death, MI, and ischemic stroke post-hsCRP measurement. Secondary outcomes included components of the primary outcome, CV death, and heart failure (HF) hospitalization. Cox regression was used to compare outcomes between patients with SI (hsCRP >2 mg/L and <10 mg/L) vs. without SI (hsCRP <2 mg/L), adjusting for demographics, comorbidities, CV treatment (statins, antiplatelets, GLP1RA, and SGLT2i), and the duration between MI and hsCRP.
Results We identified 11,230 Veterans with a nonfatal MI with a subsequent hsCRP: 3,362 had hsCRP <2 mg/L, 4,594 had hsCRP >2 mg/L and <10 mg/L, and 3,274 had hsCRP >10 mg/L. Among Veterans with hsCRP <10 mg/L, the mean age was 68 years (SD: 9.7), 96.8% were men, 73.2% had NSTEMI, and 55.6% underwent coronary revascularization. Veterans with SI were more likely to have diabetes (41.1% vs. 33.0%, p<0.001) compared to those without SI.
The composite outcome incidence was 7.2 events/100 patient-years in those with SI vs. 5.0/100 patient-years in those without SI (p<0.001). After adjustment, SI was associated with a higher risk of the primary outcome (HR: 1.31; 95% CI: 1.22–1.42). SI was also associated with an increased risk of each of the following: all-cause death, CV death, recurrent MI, and HF hospitalization (Figure 1). The results were similar after excluding patients with autoimmune disease and across subgroups by age, diabetes, heart failure, and NSTEMI vs. STEMI.
Conclusion SI following a nonfatal MI is a marker of increased risk of death, recurrent MI, and HF hospitalizations after adjustment for patient demographics, comorbidities, and CV treatment.
Sandhu, Alexander
(
Stanford University
, Millbrae , California , United States )
Furst, Adam
(
STANFORD UNIVERSITY
, Palo Alto , California , United States )
Rodriguez, Fatima
(
STANFORD UNIVERSITY
, Palo Alto , California , United States )
Kalwani, Neil
(
VA Palo Alto Health Care System
, San Carlos , California , United States )
Nallamshetty, Shriram
(
VA Palo Alto Health Care System
, San Carlos , California , United States )
Din, Natasha
(
Stanford University, VAPAHCS
, Palo Alto , California , United States )
Fan, Michael
(
Novo Nordisk
, Plainsboro, NJ , New Jersey , United States )
Khachatourian, Kat
(
Novo Nordisk
, Plainsboro, NJ , New Jersey , United States )
Skaar, Jeffrey
(
Novo Nordisk
, Plainsboro , New Jersey , United States )
Tonnu-mihara, Ivy
(
Novo Nordisk
, Plainsboro , New Jersey , United States )
Author Disclosures:
Alexander Sandhu:DO have relevant financial relationships
;
Consultant:Reprieve Cardiovascular:Active (exists now)
; Consultant:Clearly:Active (exists now)
; Research Funding (PI or named investigator):NOVO NORDISK:Active (exists now)
; Research Funding (PI or named investigator):Novartis:Active (exists now)
; Research Funding (PI or named investigator):Bayer:Active (exists now)
; Research Funding (PI or named investigator):Astra Zeneca:Active (exists now)
| Ivy Tonnu-Mihara:DO have relevant financial relationships
;
Employee:NNI:Active (exists now)
| Adam Furst:DO NOT have relevant financial relationships
| Fatima Rodriguez:DO have relevant financial relationships
;
Consultant:HealthPals:Past (completed)
; Consultant:Cleerly Health:Active (exists now)
; Consultant:Amgen:Active (exists now)
; Consultant:iRhythm:Active (exists now)
; Consultant:HeartFlow:Active (exists now)
; Consultant:Arrowhead Pharmaceuticals:Active (exists now)
; Consultant:Edwards:Active (exists now)
; Consultant:Inclusive Health:Active (exists now)
; Consultant:Esperion Therapeutics:Past (completed)
; Consultant:Kento Health:Active (exists now)
; Consultant:Movano Health:Active (exists now)
; Consultant:NovoNordisk:Past (completed)
; Consultant:Novartis:Active (exists now)
| Neil Kalwani:DO NOT have relevant financial relationships
| Shriram nallamshetty:No Answer
| Natasha Din:DO NOT have relevant financial relationships
| Michael Fan:DO have relevant financial relationships
;
Employee:Novo Nordisk:Active (exists now)
; Individual Stocks/Stock Options:Novo Nordisk:Active (exists now)
| Kat Khachatourian:DO have relevant financial relationships
;
Employee:Novo Nordisk:Active (exists now)
; Individual Stocks/Stock Options:Novo Nordisk:Active (exists now)
| Jeffrey Skaar:DO have relevant financial relationships
;
Employee:Novo Nordisk:Active (exists now)
; Individual Stocks/Stock Options:Trinity Life Sciences:Active (exists now)
; Individual Stocks/Stock Options:Novo Nordisk:Active (exists now)