Inappropriate Ventricular Fibrillation Annotation and Defibrillator Discharge During Stable Supraventricular Tachycardia: What Went Wrong?
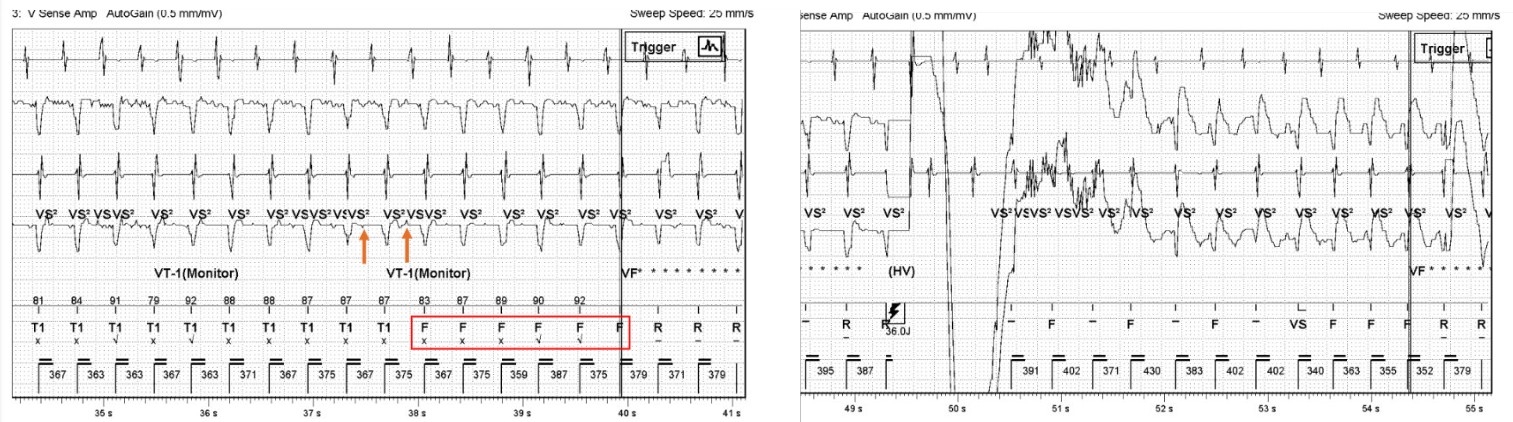
Abstract Body (Do not enter title and authors here): Background: Detection of very low amplitude ("fine") ventricular fibrillation (VF) remains a challenge for implantable cardioverter-defibrillators (ICDs), as such signals may fall below programmed sensitivity thresholds. To address this, Abbott ICDs incorporate the VF Therapy Assurance (VFTA) algorithm, which adjusts detection criteria when low-amplitude signals are sensed, aiming to reduce delayed therapy for hemodynamically unstable arrhythmias. However, this case illustrates a novel pitfall: inappropriate ICD shock triggered by misclassification of supraventricular tachycardia (SVT) as fine VF due to far-field signal distortion and VFTA activation. Case: A 53-year-old male with heart failure with recovered ejection fraction (LVEF 45–50%) from non-ischemic cardiomyopathy, paroxysmal atrial fibrillation, and an Abbott CRT-D, experienced an unexpected ICD shock while performing light housework. He had no preceding symptoms. Device interrogation revealed a regular tachycardia at 160 bpm with low-amplitude ventricular signals on the far-field Coil-Can vector. These were misclassified by the VFTA algorithm as fine VF. Once triggered, VFTA collapsed all detection zones into a single therapy zone and suppressed supraventricular discriminators. Only six ventricular beats labeled “F,” each with a cycle length faster than 400 ms, were required to fulfill VF detection criteria, and a shock was delivered. SecureSense markers showed low-amplitude R-waves annotated as “VS2,” especially before “F” annotations (Figure 1). After identifying the mechanism, the sensing vector was reprogrammed from Coil-Can to Tip-Can, improving signal fidelity and preventing recurrence. Discussion: This case highlights how VFTA, though designed to enhance VF detection, can override SVT discriminators and result in inappropriate shocks in the setting of low-amplitude far-field signals. The algorithm modifies detection criteria in response to signal dropout, but in patients with intrinsically low amplitudes, especially on far-field vectors, this may paradoxically increase misclassification risk. Reprogramming the sensing vector proved a simple and effective solution. As ICD algorithms become more sophisticated, individualized vector selection and device programming remain critical to ensuring accurate arrhythmia detection.
Shukla, Krunal
(
University of Florida
, Gainesville , Florida , United States )
Federico, Roland-austin
(
University of Florida
, Gainesville , Florida , United States )
Given, Conor
(
Abbott
, Gainesville , Florida , United States )
Bromirski, Jason
(
Abbott
, Gainesville , Florida , United States )
Xiang, Kun
(
University of Florida
, Gainesville , Florida , United States )
Author Disclosures:
Krunal Shukla:DO NOT have relevant financial relationships
| Roland-Austin Federico:No Answer
| Conor Given:DO NOT have relevant financial relationships
| Jason Bromirski:No Answer
| Kun Xiang:No Answer