Phenotyping Cardiogenic Shock Using Unsupervised Machine Learning: A Nationwide Cluster Analysis from National Inpatient Sample
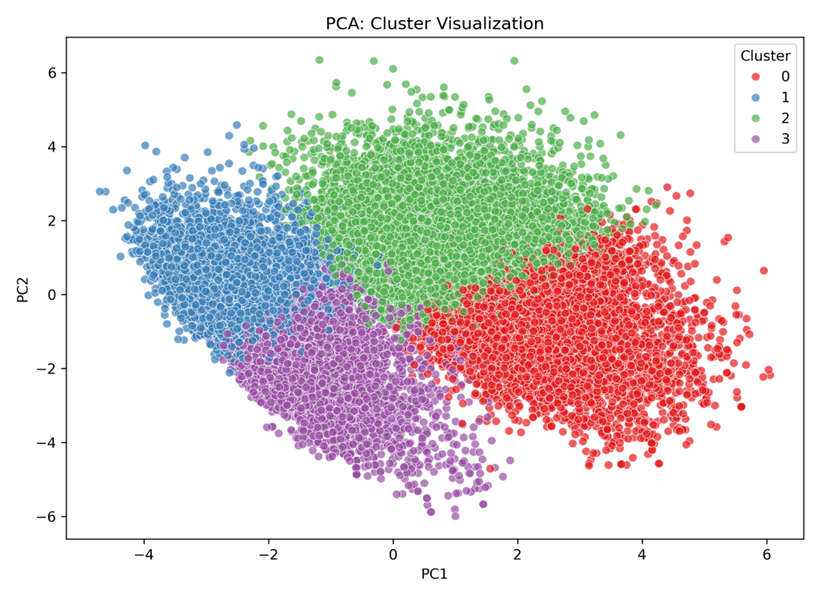
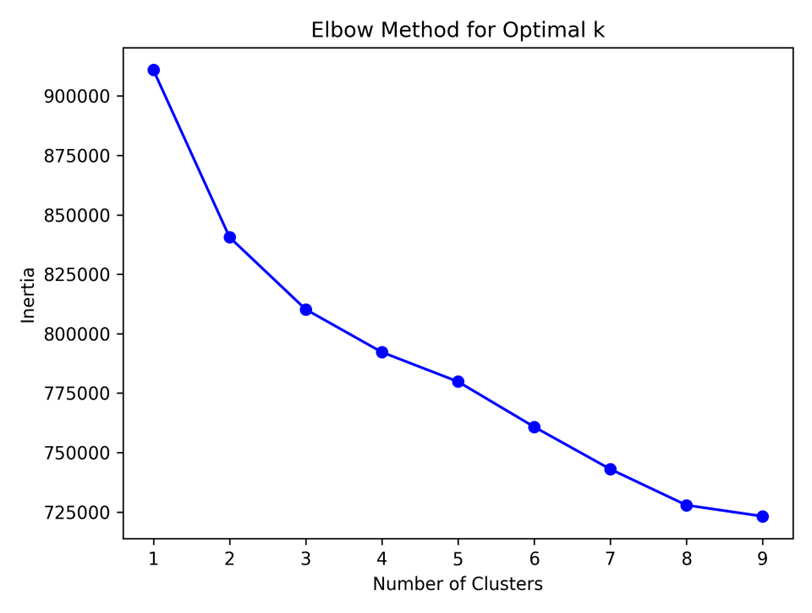
Abstract Body (Do not enter title and authors here): Introduction Cardiogenic shock (CS) is a heterogeneous clinical syndrome, with varied clinical outcomes driven by hemodynamic states, and initial presentation. However, unsupervised machine learning (ML) has not been implemented to identify clinically meaningful subgroups to improve risk stratification and therapeutic targeting ina nationally representative sample. Methods We used the 2016–2019 National Inpatient Sample (NIS) to identify non-elective hospitalizations with CS without prior heart transplant. Density-Based Spatial Clustering of Applications with Noise (DBSCAN) was applied to 14 clinical covariates including procedures, and comorbidity burden scores (Elixhauser Comorbidity and CHA2DS2Vasc). The primary outcome was in-hospital mortality. Secondary outcomes included use of mechanical circulatory support (MCS), invasive mechanical ventilation, hemodialysis, and major complications. Multivariable logistic regression was used to assess mortality and outcomes. Feature importance was interpreted using SHapley Additive exPlanations (SHAP) values. Results Among 91,131 unweighted CS hospitalizations, four distinct clusters were identified: Cluster 0 (37.6%): Older adults with multiple comorbidities, highest CHA2DS2Vasc burden, frequent use of invasive ventilation and hemodialysis. Cluster 1 (32.7%): Predominantly ischemic CS with high rates of PCI/CABG, younger population, and lowest mortality. Cluster 2 (16.4%): Critically ill patients with multiorgan failure, sepsis, transfusion, dialysis, and the highest in-hospital mortality (48.9%). Cluster 3 (13.3%): Patients with prior CABG and atrial fibrillation, frequent use of early RHC but lower revascularization. MCS utilization was most frequent in Cluster 2 (37.2%), followed by Cluster 1 (32.1%). Mortality varied significantly across phenotypes (p < 0.001). After adjustment, Clusters 2 and 0 had significantly higher odds of mortality compared to Cluster 1 (aOR 2.42 [95% CI 2.30–2.56] and 1.68 [95% CI 1.59–1.77], respectively). SHAP analysis revealed age, mechanical ventilation, sepsis, and dialysis as key predictors of mortality. Conclusion Unsupervised ML identified four clinically distinct phenotypes of CS, utilizing various treatment modalities with differing outcomes. Cluster 2, characterized by multiorgan failure and highest MCS use, had the worst prognosis. These data driven phenotypes may guide clinicians for future risk stratification and guide precautionary measures to manage CS.
Mondal, Avilash
(
West Virginia University
, Morgantown , West Virginia , United States )
Haider, Mobeen
(
West Virginia University
, Morgantown , West Virginia , United States )
Thyagaturu, Harshith
(
West Virginia University
, Morgantown , West Virginia , United States )
Taha, Amro
(
West Virginia University
, Morgantown , West Virginia , United States )
Li, Aobo
(
Inspira Health Vineland
, Glassboro , New Jersey , United States )
Chilingarashvili, Giorgi
(
Nazareth Hospital
, Philadelphia , Pennsylvania , United States )
Ramesh, Ranjana
(
Brown University
, North Chelmsford , Massachusetts , United States )
Ramesh, Navin
(
Brown University
, N Chelmsford , Massachusetts , United States )
Balla, Sudarshan
(
West Virginia University
, Morgantown , West Virginia , United States )
Tripathi, Devendra
(
Nazareth Hospital
, Philadelphia , Pennsylvania , United States )
Author Disclosures:
Avilash Mondal:DO NOT have relevant financial relationships
| Devendra Tripathi:DO NOT have relevant financial relationships
| Mobeen Haider:DO NOT have relevant financial relationships
| Harshith Thyagaturu:DO NOT have relevant financial relationships
| Amro Taha:DO NOT have relevant financial relationships
| Aobo Li:DO NOT have relevant financial relationships
| Giorgi Chilingarashvili:DO NOT have relevant financial relationships
| Ranjana Ramesh:DO NOT have relevant financial relationships
| Navin Ramesh:DO NOT have relevant financial relationships
| sudarshan balla:DO NOT have relevant financial relationships