Pulmonary Hypertension is associated with higher In-Hospital Complications After Transcatheter Mitral Valve Intervention- A Nationwide Analysis of 73,000 Patients
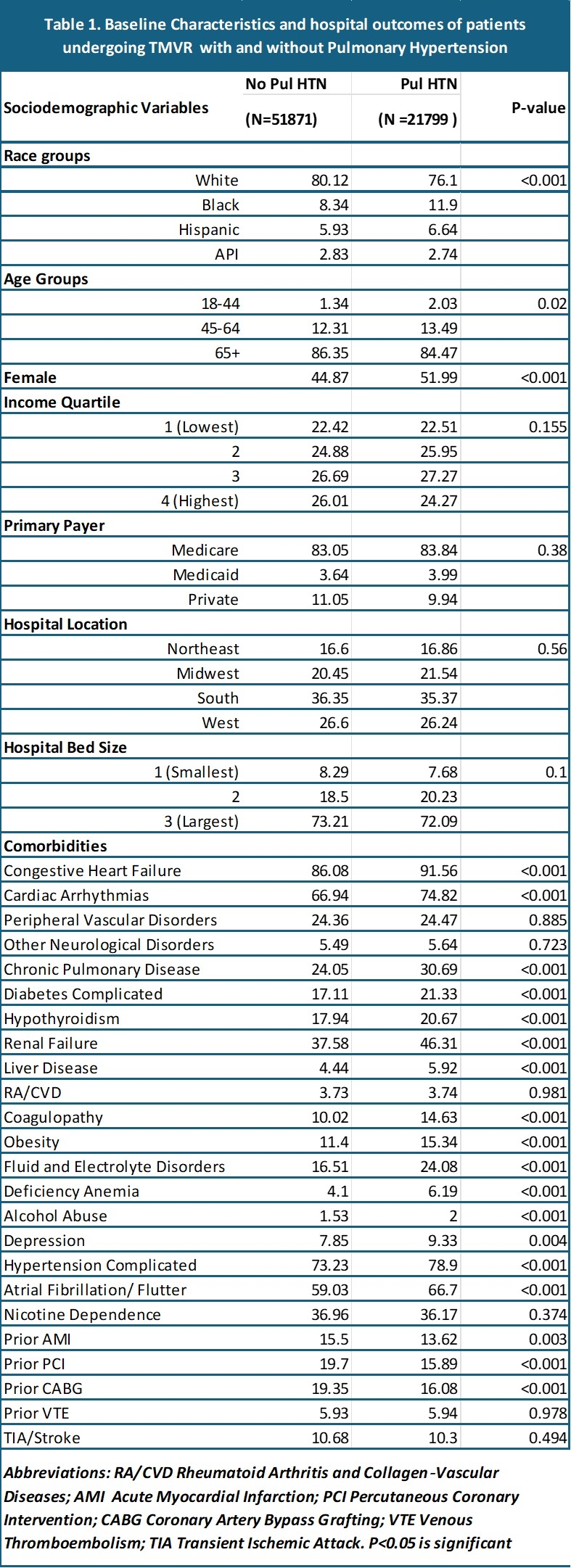
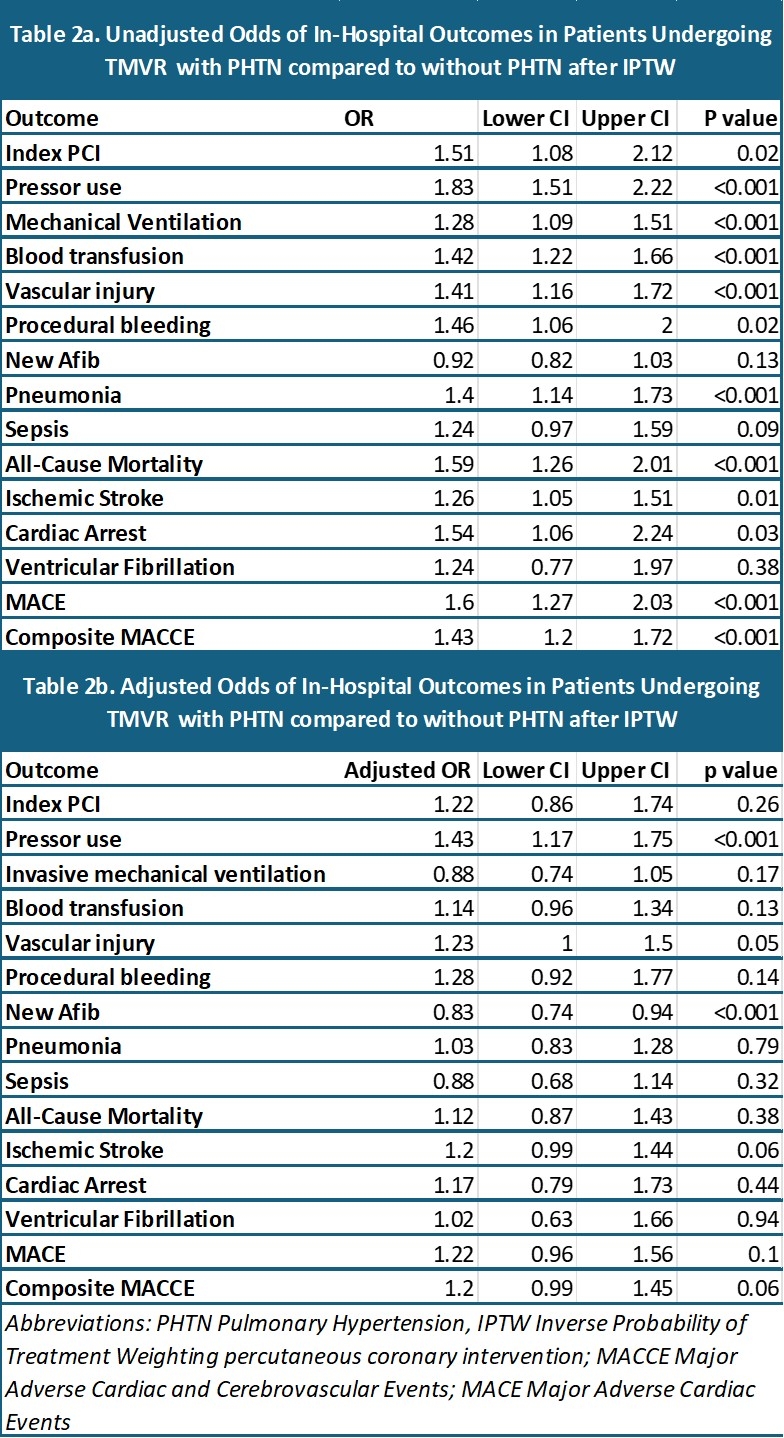
Abstract Body (Do not enter title and authors here): Background Pulmonary hypertension (PH) is commonly associated with mitral valve disease. Transcatheter mitral valve repair (TMVR), involves transseptal approach to replace the diseased mitral valve, but its impact on periprocedural outcomes is not explored in the PHTN group. Methods We performed a retrospective study of adults undergoing TMVR using the National Inpatient Sample (2016–2022). Patients were stratified by documented PH. Inverse probability of treatment weighting (IPTW) was used on propensity scores (PS). Excellent covariate balance (standardized mean differences(SMD) <10%) and overlap were achieved(Fig 1). Multivariate logistic regression was used to obtain adjusted odds ratios (aORs) for in-hospital primary (all-cause mortality) and secondary outcomes (including stroke, cardiac arrhythmias, acute kidney injury, procedural complications and major adverse cardiovascular events) after adjusting for gender, heart failure, cardiac arrhythmias, diabetes, hypertention prior PCI and CABG for possible confounders based on SMD plot. P<0.05 was considered statistically significant. Results Among 73, 670 weighted TMVR admissions (21,799 PH; 51,871 without PH;), the PH cohort more often comprised of females and had higher burden of comorbid conditions (all P<0.05) (Table 1). In unadjusted IPTW analyses, PH was associated with higher odds of index PCI (OR 1.51; 95% CI 1.08–2.12), pressor use (1.83; 1.51–2.22), mechanical ventilation (1.28; 1.09–1.51), blood transfusion (1.42; 1.22–1.66), vascular injury (1.41; 1.16–1.72), procedural bleeding (1.46; 1.06–2.00), pneumonia (1.40; 1.14–1.73), all-cause mortality (1.59; 1.26–2.01), ischemic stroke (1.26; 1.05–1.51), cardiac arrest (1.54; 1.06–2.24), MACE (1.60; 1.27–2.03), and composite MACCE events(1.43; 1.20–1.72) (all p<0.05)(Table 2a). After multivariable adjustment, PH groups had higher odds of pressor use (aOR 1.43; 1.17–1.75; P<0.001),but reduced risk of new atrial fibrillation (0.83; 0.74–0.94; P<0.001).No significant adjusted differences were observed for mortality, MACE, or other complications after adjustment (Table 2b). Conclusions In TMVR patients, PH predicts greater need for hemodynamic support and is paradoxically linked to lower new onset atrial fibrillation but does not independently increase in hospital mortality or MACE. These findings highlight the importance of optimizing peri procedural management in PH cohorts and curtail worse outcomes in high-risk population groups.
Razdan, Nandini
(
Reading Hospital, Tower Health
, Pennsylvania , Pennsylvania , United States )
Mondal, Avilash
(
West Virginia University
, Morgantown , West Virginia , United States )
Green, Jared
(
Reading Hospital, Tower Health
, Pennsylvania , Pennsylvania , United States )
Diaz Fraga, Julian
(
Reading Hospital, Tower Health
, Pennsylvania , Pennsylvania , United States )
Basnet, Arjun
(
Reading Hospital, Tower Health
, Pennsylvania , Pennsylvania , United States )
Li, Aobo
(
Inspira Health Vineland
, Glassboro , New Jersey , United States )
Fagan, James
(
PCOM
, Philadelphia , Pennsylvania , United States )
Chilingarashvili, Giorgi
(
Nazareth Hospital
, Philadelphia , Pennsylvania , United States )
Prasad, Abhishek
(
Duke University Medical Center
, Houston , Texas , United States )
Singh, Aniruddha
(
Reading Hospital, Tower Health
, Pennsylvania , Pennsylvania , United States )
Author Disclosures:
Nandini Razdan:No Answer
| Aniruddha Singh:No Answer
| Avilash Mondal:DO NOT have relevant financial relationships
| Jared Green:No Answer
| Julian Diaz Fraga:No Answer
| Arjun Basnet:DO NOT have relevant financial relationships
| Aobo Li:DO NOT have relevant financial relationships
| James Fagan:DO NOT have relevant financial relationships
| Giorgi Chilingarashvili:DO NOT have relevant financial relationships
| Abhishek Prasad:DO NOT have relevant financial relationships