Where Is My Valve? Three-Decade Survival for Tricuspid Valvectomy Without Valve Replacement Following Infective Endocarditis
Abstract Body (Do not enter title and authors here):
Background: Amid the opioid pandemic, rising intravenous drug use (IVDU) has markedly increased the incidence of tricuspid valve endocarditis (TVE), a serious complication. While long-term IV antibiotics are the mainstay treatment, refractory cases may require surgery. Tricuspid valvectomy without prosthetic replacement is a rare option, chosen in select cases to reduce reinfection risk and support recovery from IVDU. However, this approach can cause chronic right heart volume overload, right atrial enlargement, and atrial fibrillation, leading to eventual valve replacement in a large number of cases.
Case report: We report a rare case of a 61-year-old male with a longstanding history of IVDU who presented with progressive shortness of breath and peripheral edema, 32 years following isolated tricuspid valvectomy without valve replacement performed for refractory tricuspid valve endocarditis (TVE). His past medical history included COPD on home oxygen therapy, paroxysmal atrial flutter, and heavy tobacco use.
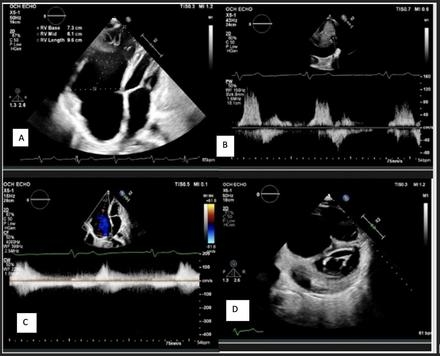
Clinical examination revealed signs consistent with chronic venous congestion, including bilateral lower extremity edema and elevated jugular venous distention. Echocardiography assessment demonstrated preserved left ventricular ejection fraction (65%), markedly dilated right atrium and ventricle (ventricularization of the right atrium), absence of the tricuspid valve, and elevated central venous pressure. Due to underlying COPD, initial respiratory management led to clinical improvement, and the patient was discharged for outpatient cardiopulmonary follow-up. We decided against valve replacement during his clinic visit, given his medical history and ability to perform all daily activities independently without any symptoms.
Discussion: This report underscores the remarkable feasibility of prolonged survival following tricuspid valvectomy without prosthetic replacement. Despite significant anatomical changes, including marked right-heart chamber dilation, severe right heart failure was notably absent even decades post-surgery. It challenges traditional surgical paradigms and suggests that conservative management may remain viable decades after valvectomy, calling for more nuanced decision-making frameworks. Our findings underscore the need for standardized guidelines and long-term echocardiographic surveillance in patients post-valvectomy to identify subtle signs of decompensation and optimize timing for potential intervention.
Vadnagara, Harsh
(
B. J. Medical College, Ahmedabad
, Ahmedabad , India )
Garg, Vasudha
(
B. J. Medical College, Ahmedabad
, Ahmedabad , India )
Momin, Elina
(
Louisiana State University Shreveport
, Shreveport , Louisiana , United States )
Momin, Aryan
(
NHL Medical College
, Ahmedabad , Gujarat , India )
Tayeb, Taher
(
Louisiana State University Shreveport
, Shreveport , Louisiana , United States )
Author Disclosures:
HARSH VADNAGARA:DO NOT have relevant financial relationships
| Vasudha Garg:DO NOT have relevant financial relationships
| Elina Momin:No Answer
| Aryan Momin:No Answer
| Taher Tayeb:No Answer