CAUGHT IN THE NET: A RARE CASE OF MRSA ENDOCARDITIS OF THE CHIARI NETWORK
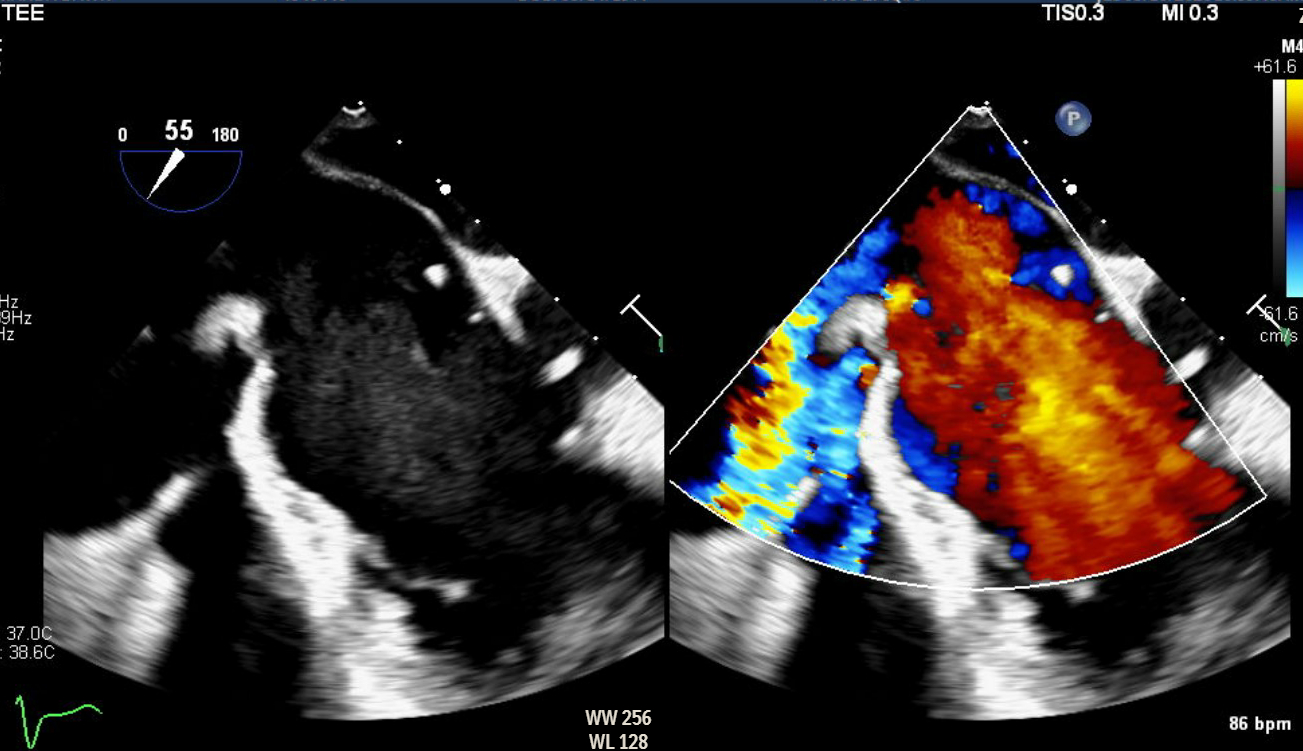
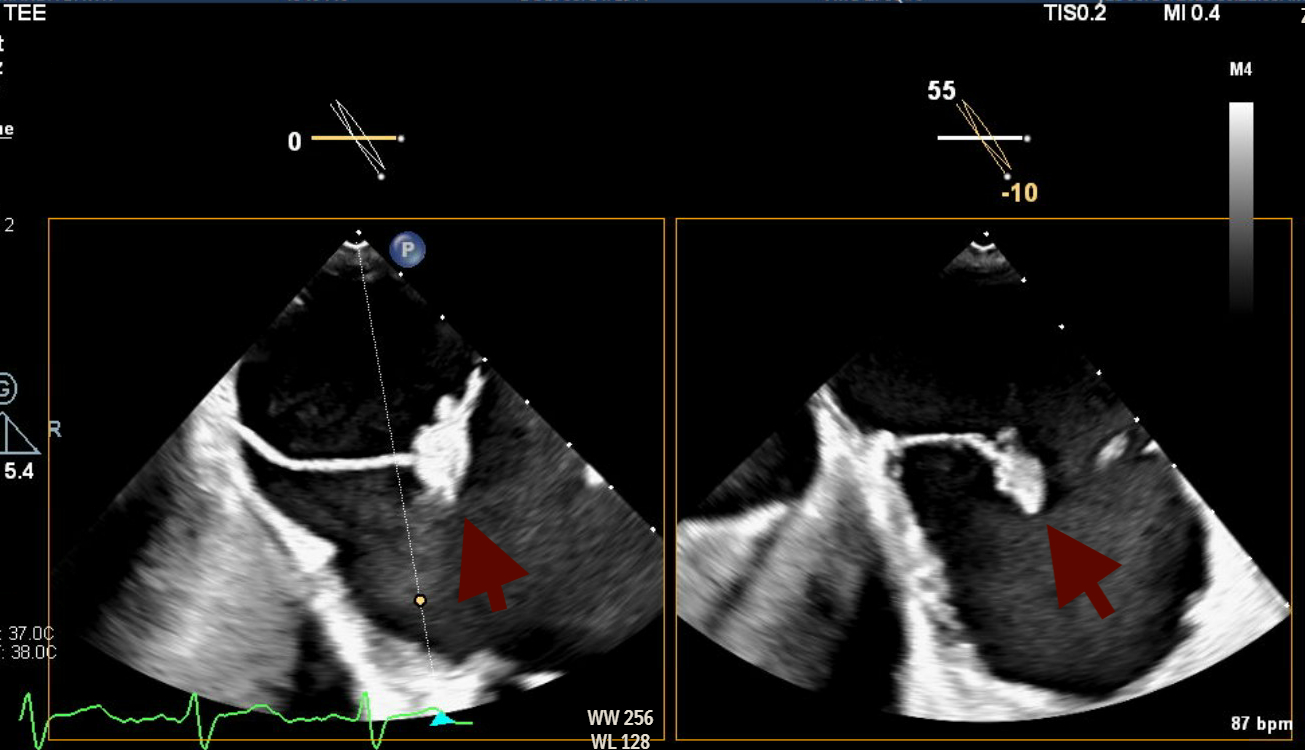
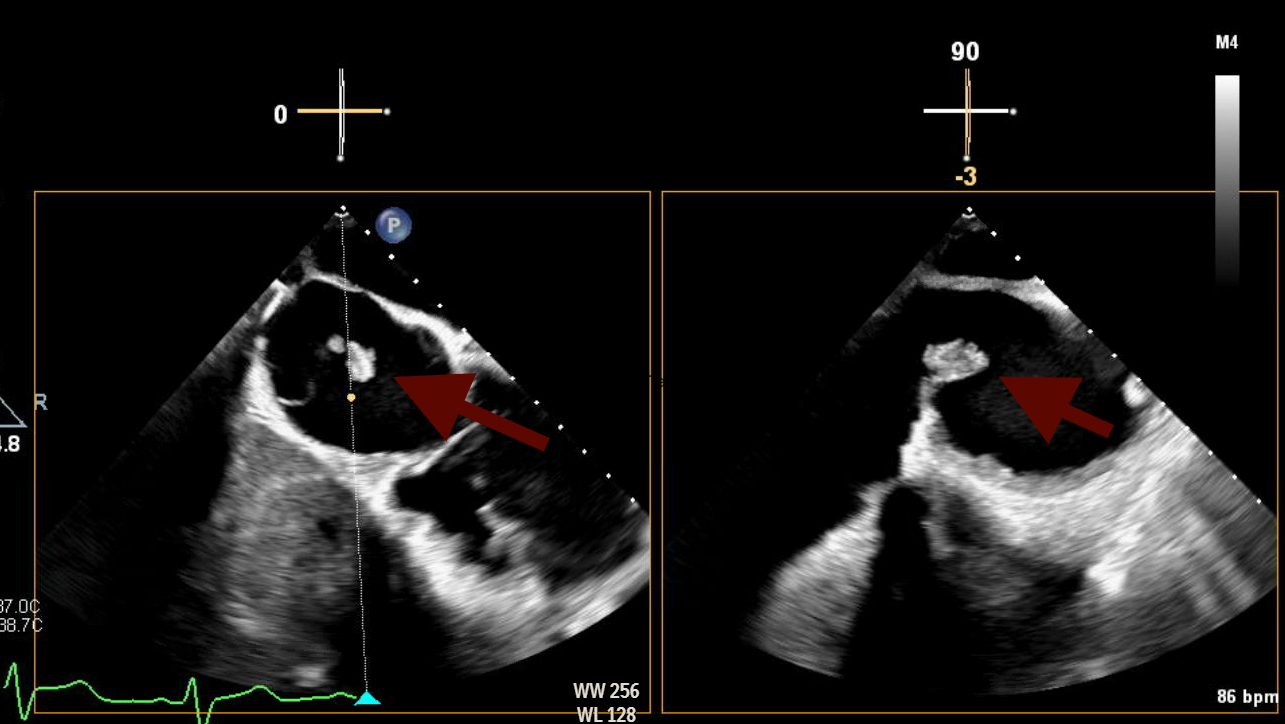
Abstract Body (Do not enter title and authors here): Here is a rare and diagnostically challenging case of infective endocarditis (IE) involving the Chiari network in a 47-year-old female with a complex cardiac and social history. She had a history of intravenous drug use (IVDU), prior methicillin-sensitive Staphylococcus aureus (MSSA) bacteremia involving the mitral valve (MV), and methicillin-resistant Staphylococcus aureus (MRSA) endocarditis requiring tricuspid valve (TV) replacement with a CorMatrix bioprosthesis. She presented with a 3-day history of fever, progressive right groin pain and swelling, and worsening dyspnea. On admission, she was afebrile but hypotensive and had tachycardia. On examination, she had a loud holosystolic murmur in the left lower sternal border, a pulsatile right groin mass with a bruit, alongside multiple healed track marks on her lower extremities. Blood work was notable for leukocytosis. Computed tomography of the chest, abdomen, and pelvis revealed multiple pulmonary septic emboli and a right femoral artery pseudoaneurysm with an arteriovenous fistula confirmed on duplex ultrasound. Transthoracic echocardiogram (TTE) showed preserved ejection fraction (60-65%), normal aortic and mitral valves, but poor visualization of the prosthetic tricuspid valve. Blood cultures grew MRSA, and the patient was started on IV vancomycin. Transesophageal echocardiogram (TEE) revealed a large, mobile echogenic mass attached to the Chiari network (CN), positioned in line with the tricuspid regurgitant jet. These new findings, absent on prior imaging, strongly suggested isolated Chiari network endocarditis (CNE) Right-sided infective endocarditis (IE) is a rare clinical entity, accounting for less than 10% of all IE cases. Among these, involvement of the CN- the embryonic remnant of the right valve of the sinus venosus and present in under 2% of the population- is even rarer, with only a few reported cases to date. IVDU remains the leading risk factor for right-sided IE, as seen in our patient. The true incidence of CNE is likely underreported due to the limited sensitivity of TTE, which can make visualizing it challenging. TEE remains the imaging modality of choice for identifying such atypical presentations. Our case reinforced the critical role of TEE in identifying uncommon, non-valvular sources of infection. In the absence of clear treatment guidelines and high surgical risk, the patient was treated conservatively with a 6-week course of antibiotics followed by repeat TEE for monitoring.
Subramanian, Lakshmi
(
East Carolina University Health
, Greenville , North Carolina , United States )
Udani, Kunjan
(
East Carolina University Health
, Greenville , North Carolina , United States )
Srikanth, Sashwath
(
East Carolina University Health
, Greenville , North Carolina , United States )
Alrubaye, Lara
(
ECU Health Medical Center
, Winterville , North Carolina , United States )
Ardhanari, Sivakumar
(
East Carolina University
, Cary , North Carolina , United States )
Author Disclosures:
Lakshmi Subramanian:DO NOT have relevant financial relationships
| Kunjan Udani:DO NOT have relevant financial relationships
| Sashwath Srikanth:DO NOT have relevant financial relationships
| Lara Alrubaye:DO NOT have relevant financial relationships
| Sivakumar Ardhanari:No Answer