Primary non-adherence and patterns of underutilization of guideline-directed medical therapy following hospitalizations for myocardial infarction
Abstract Body (Do not enter title and authors here): Background Guideline-directed medical therapy (GDMT) following a myocardial infarction (MI) is crucial for secondary prevention. Prescription of GDMT is emphasized at hospital discharge, but GDMT adherence and persistence following the initial prescription are often overlooked.
Methods Retrospective cohort study of electronic health records from a 40-hospital US health system. We included adults hospitalized for MI and discharged home between 1/2018-9/2022. We measured GDMT as treatment with beta-blockers (BBs), renin-angiotensin-aldosterone system inhibitors (RAASis), high-intensity statins, and P2Y12 inhibitors. We categorized use of each GDMT class as continuation (fills prior to hospitalization), initiation (a new fill within 7 days of discharge), or primary non-adherence (new prescription at discharge, but absence of a fill). Among continuers and initiators, we defined secondary adherence at 12 months as proportion of days covered (PDC) ≥80% and persistence as continuous days’ supply at 12 months with 90 day grace periods. We tested differences in persistence by continuation vs initiation and by STEMI vs NSTEMI using log-rank tests.
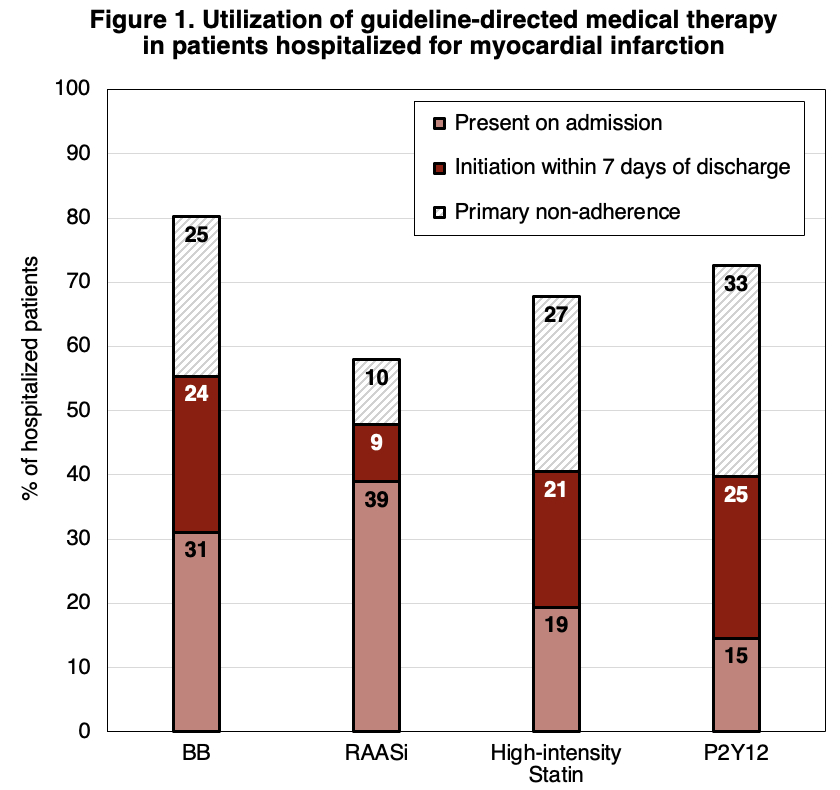
Results The cohort included 5265 MI hospitalizations (age 68 (IQR 77-60) years, 39% female, 91% White, 7% Black, 75% NSTEMI). Among those without use prior to admission, 71%, 31%, 60%, and 68% of patients were newly prescribed BBs, RAASis, statins, and P2Y12s, respectively, at discharge (Figure 1).
However, 54% of new prescriptions for GDMT were unfilled by 7 days post-discharge, indicating primary non-adherence. In total, only 55%, 48% 41%, and 40% of patients continued or initiated BBs, RAASis, statins, and P2Y12s at discharge, respectively. As a result, 14% of patients received all four GDMT medications at discharge.
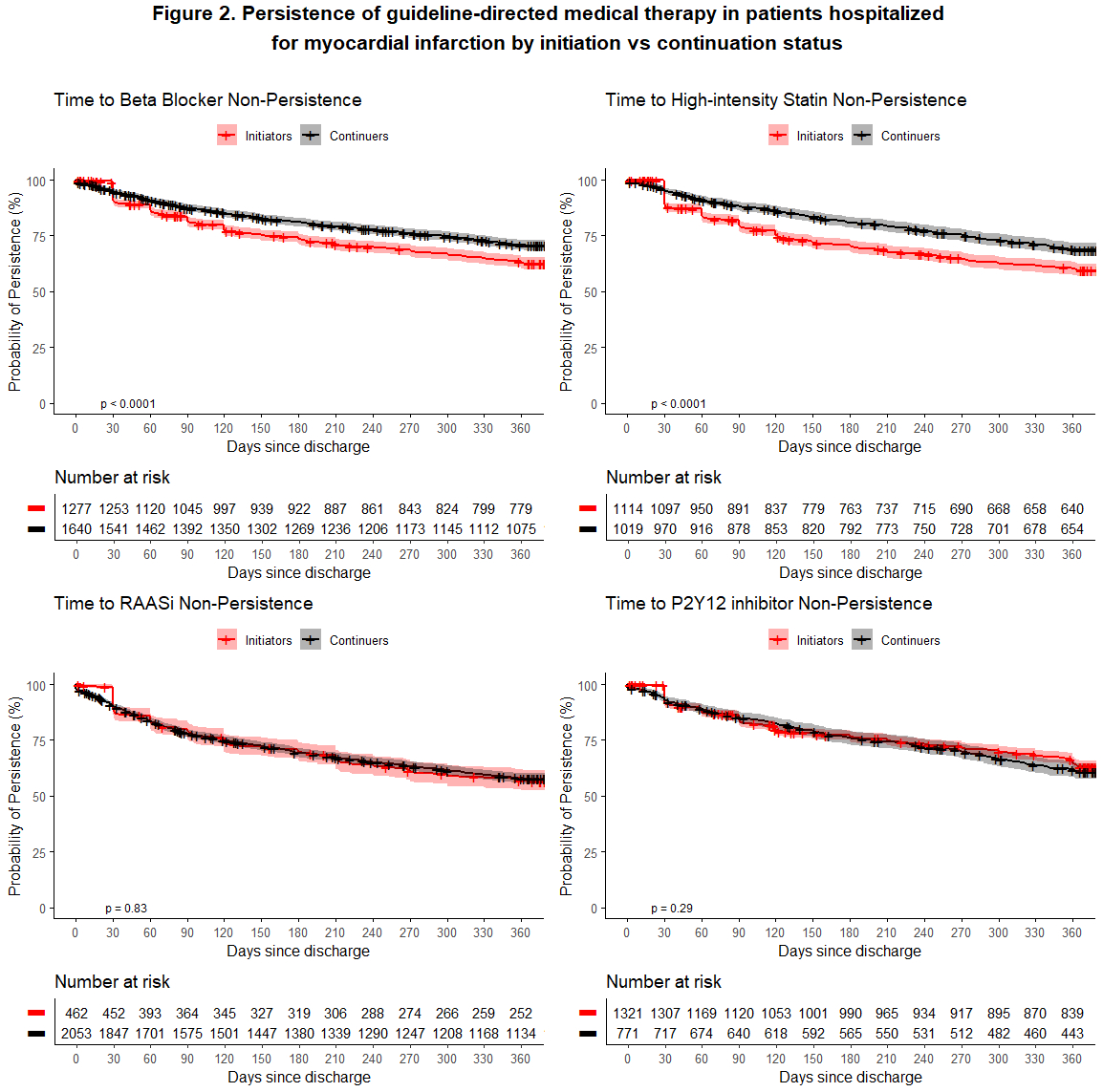
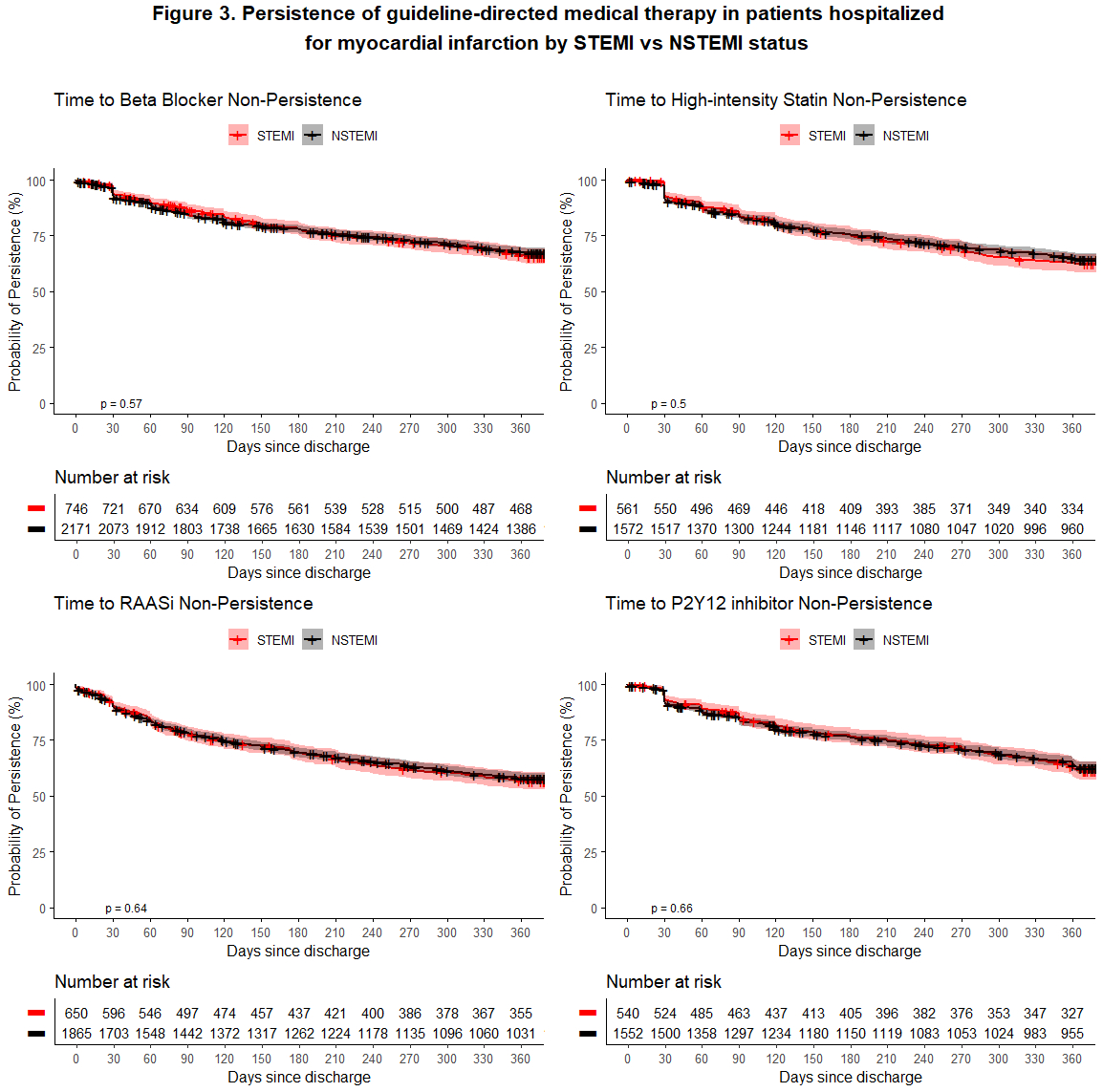
At 12 months post-discharge, 58% were adherent and 48% were persistent to all discharge GDMT medications. Differences in persistence of BBs and statins were observed by initiation status, but not for RAASis or P2Y12s (Figure 2). There were no significant differences in GDMT persistence between patients with STEMI vs NSTEMI (Figure 3).
Conclusions In our cohort, over half of GDMT prescriptions for secondary prevention following an MI hospitalization went unfilled, and only half of patients were adherent or persistent to GDMT in the year following an MI hospitalization. These results emphasize the need for interventions to support medication adherence following transitions in the post-discharge period.
Bessette, Lily
(
University of Pittsburgh
, Pittsburgh , Pennsylvania , United States )
Mayrer, Bridget
(
University of Pittsburgh
, Pittsburgh , Pennsylvania , United States )
Magnani, Jared
(
University of Pittsburgh
, Pittsburgh , Pennsylvania , United States )
Brooks, Maria
(
University of Pittsburgh
, Pittsburgh , Pennsylvania , United States )
Anderson, Timothy
(
University of Pittsburgh
, Pittsburgh , Pennsylvania , United States )
Author Disclosures:
Lily Bessette:DO NOT have relevant financial relationships
| Bridget Mayrer:DO NOT have relevant financial relationships
| Jared Magnani:DO NOT have relevant financial relationships
| Maria Brooks:No Answer
| Timothy Anderson:DO NOT have relevant financial relationships