Superior Vena Cava Isolation Combined with Pulmonary Vein Isolation versus Pulmonary Vein Isolation Alone in Atrial Fibrillation Ablation: A Meta-Analysis of Randomized Controlled Studies with Trial Sequential Analysis
Abstract Body (Do not enter title and authors here): Background: Pulmonary vein isolation (PVI) is standard in atrial fibrillation (AF) ablation, but recurrence remains common. Non-pulmonary triggers, especially from the superior vena cava (SVC), may contribute. The role of adding SVC isolation is unclear due to limited and conflicting trial data.
Methods: PubMed, Scopus, Embase, Web of Science, and Cochrane were systematically searched up to May 2025 to identify studies comparing SVC isolation combined with PVI versus PVI alone in AF ablation. Dichotomous data were pooled using the inverse variance method under a fixed-effect model and reported as odds ratios (ORs) with 95% CIs. Continuous data were pooled using the inverse variance method under a random-effects model and reported as mean differences (MDs) with 95% CIs. Trial sequential analysis (TSA) was conducted for primary outcomes to assess the risks of Type I and Type II errors. All analyses were performed using the appropriate packages in R software version 4.3.2.
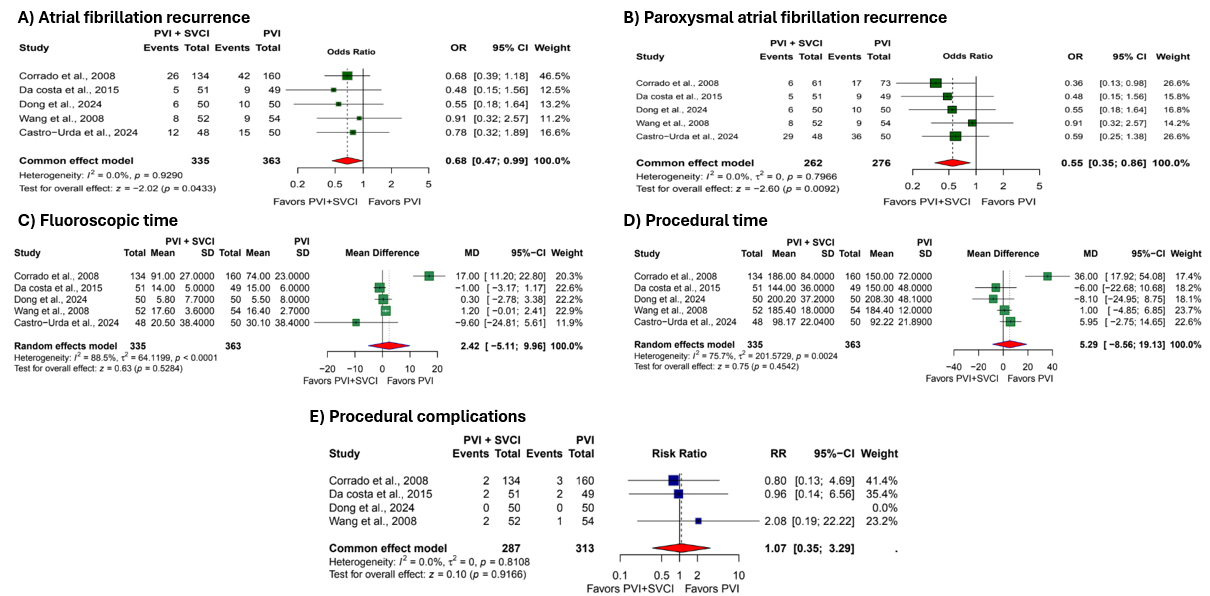
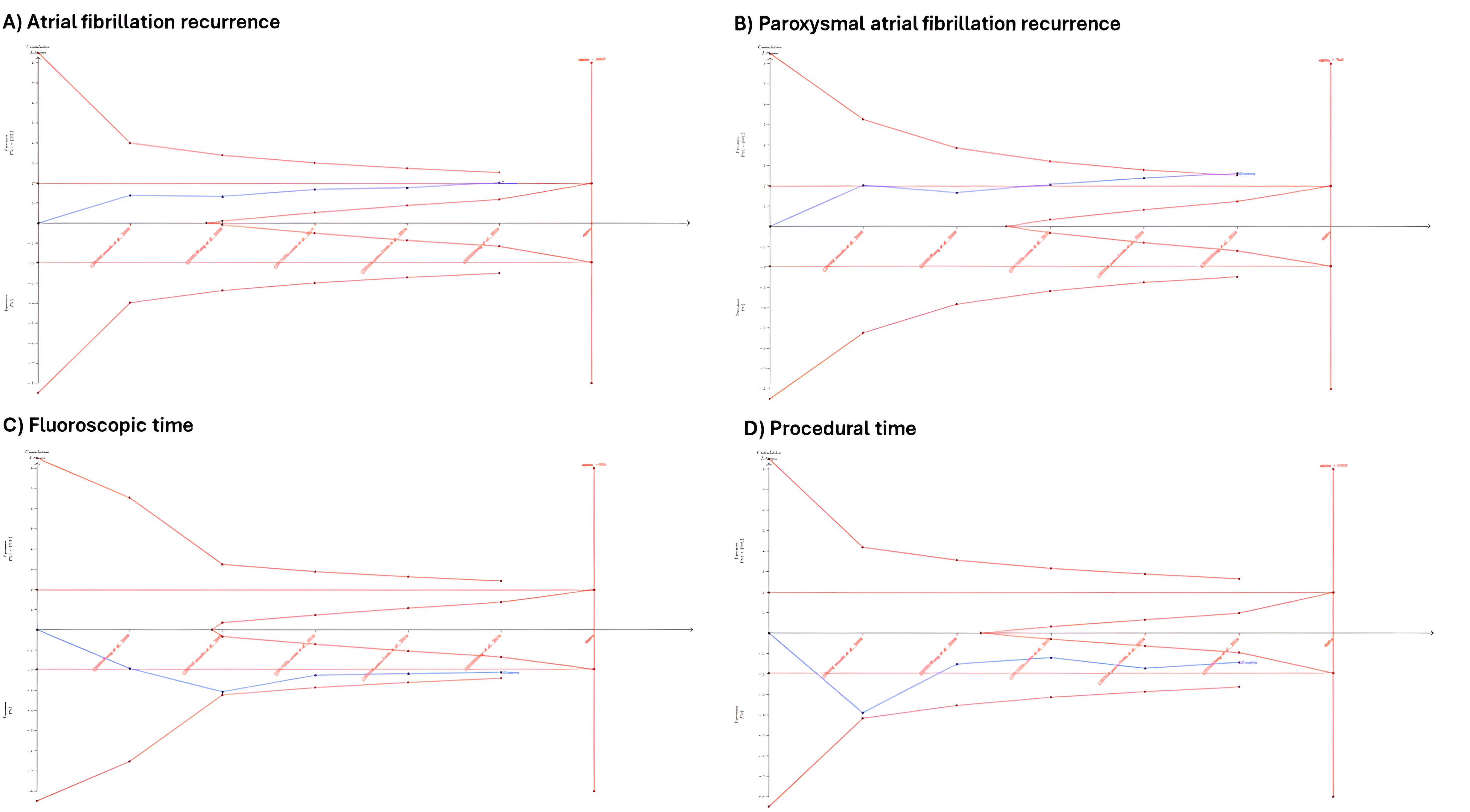
Results: Five RCTs comprising 700 patients (PVI + SVCI: 337; PVI alone: 363) were included in the analysis. Combined PVI and SVCI was associated with a significantly lower risk of total AF recurrence (OR: 0.68; 95% CI: 0.47, 0.99; p=0.04) and paroxysmal AF recurrence (OR: 0.55; 95% CI: 0.35, 0.86; p=0.009). No significant differences were observed between groups in fluoroscopy time (min) (MD = 2.42; 95% CI: –5.11, 9.96; p=0.52), procedural duration (min) (MD = 5.29; 95% CI: –8.56, 19.13; p=0.45), or complication rates (OR: 1.07; 95% CI: 0.35, 3.29; p= 0.91). TSA confirmed conclusive evidence only for fluoroscopic time, while outcomes for AF recurrence, paroxysmal AF recurrence, and procedural time remained statistically inconclusive.
Conclusion: In patients undergoing AF ablation, the addition of SVC isolation to standard PVI significantly reduces the recurrence of AF, particularly for paroxysmal AF. However, this benefit is tempered by TSA, which reveals insufficient cumulative evidence to draw definitive conclusions for most outcomes. The reduction in fluoroscopic time is statistically conclusive, but no procedural or safety advantage was observed. These findings suggest a potential role for SVC isolation in select patients, but larger, adequately powered trials are required to validate its routine application.
Odat, Ramez
(
Jordan University of Science and Technology
, Irbid , Jordan )
Aldamen, Ali
(
Yarmouk University
, Irbid , Jordan )
Aldamen, Raneem
(
The Hashemite University
, Zarqa , Jordan )
Altarawneh, Tala
(
Marshall University
, Huntington , West Virginia , United States )
Soni, Kriti
(
SUNY Upstate Medical University
, Syracuse , New York , United States )
Khan, Rozi
(
HCA Houston Healthcare/University of Houston
, Houston , Texas , United States )
Patel, Bhavin
(
Cape Fear Valley Hospital
, Fayetteville , North Carolina , United States )
Jain, Hritvik
(
AIIMS Jodhpur
, Jodhpur , India )
Gharaibeh, Ahmad
(
Boston University
, Boston , Massachusetts , United States )
Author Disclosures:
Ramez Odat:DO NOT have relevant financial relationships
| Ahmad Gharaibeh:No Answer
| Ali Aldamen:DO NOT have relevant financial relationships
| Belal Hamed:No Answer
| Raneem Aldamen:No Answer
| Tala Altarawneh:No Answer
| Kriti Soni:DO NOT have relevant financial relationships
| Rozi Khan:DO NOT have relevant financial relationships
| Bhavin Patel:DO NOT have relevant financial relationships
| Hritvik Jain:DO NOT have relevant financial relationships