Low prevalence of coronary and thoracic aortic calcium in high-cardiometabolic risk Kenyan adults with and without HIV: The ASANTE Study
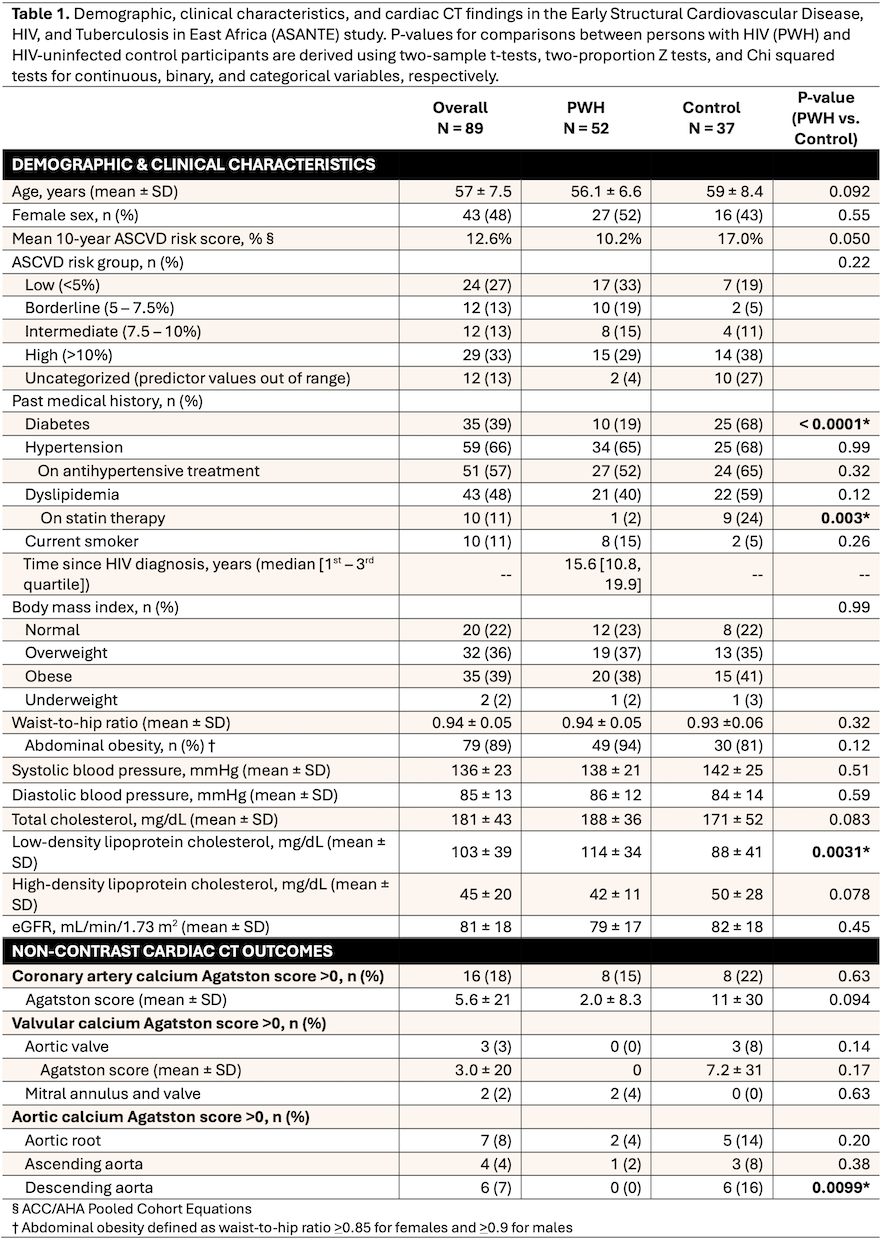
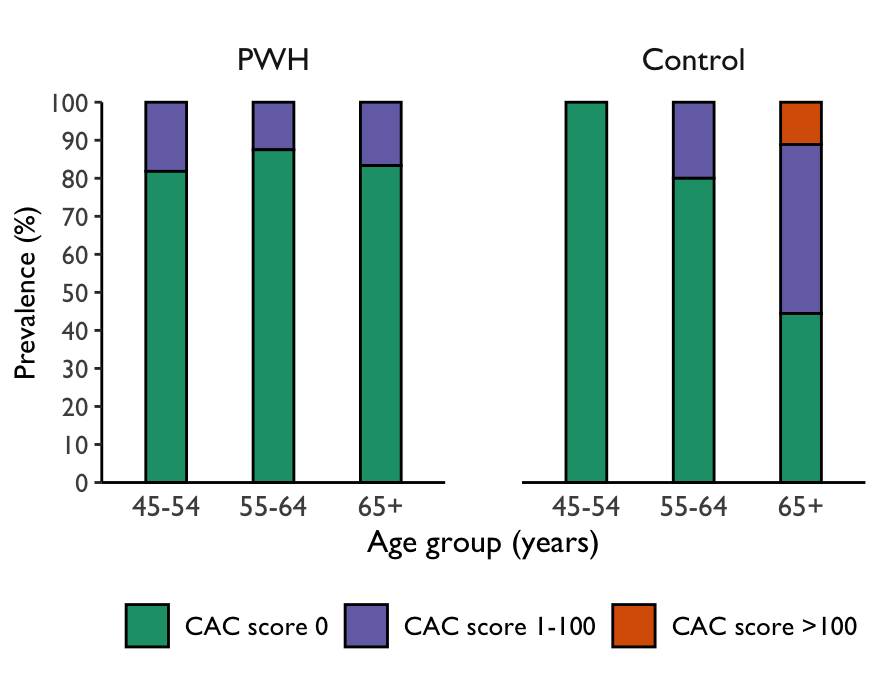
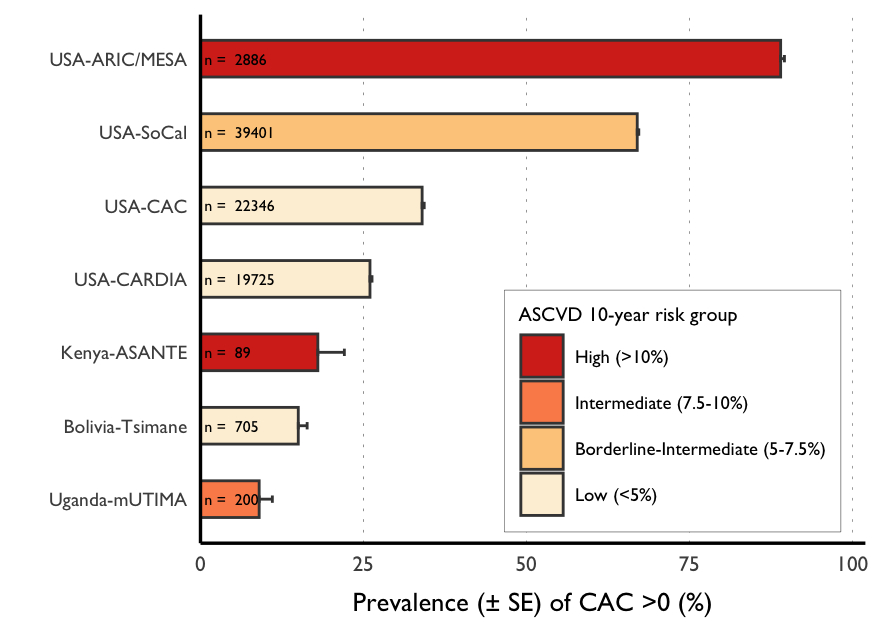
Abstract Body (Do not enter title and authors here): Background: HIV is thought to be an independent risk factor for atherosclerotic cardiovascular disease (ASCVD), including coronary atherosclerosis, based on studies from high-income countries. However, there are limited data on the epidemiology of atherosclerosis from sub-Saharan Africa, where there is a high burden of HIV. Methods: Early Structural Cardiovascular Disease, HIV, and Tuberculosis in East Africa (ASANTE) is an ongoing cross-sectional study evaluating coronary atherosclerosis in Kenyan adults with chronically treated/suppressed HIV (PWH) and HIV-uninfected controls. We enroll participants >45 years old with >1 cardiometabolic risk factor (hypertension, diabetes, dyslipidemia, smoking, overweight/obesity), targeting a sample of n = 200 (50% female, 50% PWH). Participants undergo comprehensive exposure assessments and non-contrast cardiac CT. We quantify coronary artery calcium (CAC) as a measure of coronary atherosclerosis, thoracic aortic calcium (TAC), and valvular calcium using Agatston scores. We report interim results on clinical characteristics, CAC, TAC, and valvular calcium. We also compare CAC prevalence and estimated 10-year ASCVD risk in ASANTE to other published geographic cohorts. Results: We included 52 PWH and 37 HIV-uninfected control participants who completed CT imaging in this analysis (Table 1). The mean age among all participants was 57 years, and 48% were female. The mean 10-year ASCVD risk score was 12.6% (10.2% in PWH, 17% in controls). Prevalence of diabetes and statin therapy for hyperlipidemia was higher among controls (p < 0.01), while low-density lipoprotein levels were higher among PWH (p = 0.003). Prevalence of CAC >0 by Agatston score was 18% (15% in PWH, 22% in controls; p = 0.63). Prevalence of CAC scores by category are shown in Figure 1. Valvular and thoracic aortic calcium prevalence was lower than CAC, ranging from 2% to 8% among all participants. Despite having high mean 10-year cardiovascular risk, ASANTE participants had lower CAC prevalence compared with lower-risk cohorts in the United States (p = 0.02 and p <0.001 for ASANTE vs. USA-CAC Consortium and ASANTE vs. USA-SoCal, respectively; Figure 2). Conclusion: Despite enriching for cardiovascular risk factors, CAC is less common in the East African population, regardless of HIV status, compared with lower-risk cohorts in high-income settings. Further studies are needed to identify potential atheroprotective exposures and mechanisms in this region.
Krishnan, Srikanth
(
University of California Los Angeles
, Los Angeles , California , United States )
Narashim, Aditya
(
University of California Los Angeles
, Los Angeles , California , United States )
Kipkorir, Sidney
(
Kenyatta National Hospital
, Nairobi , Kenya )
Omondi, Geoffrey
(
Kenyatta National Hospital
, Nairobi , Kenya )
Ale, Boni
(
University of Nairobi
, Nairobi , Kenya )
Gitura, Bernard
(
Kenyatta National Hospital
, Nairobi , Kenya )
Kinuthia, John
(
Kenyatta National Hospital
, Nairobi , Kenya )
Farquhar, Carey
(
University of Washington
, Seattle , Washington , United States )
Hsue, Priscilla
(
University of California Los Angeles
, Los Angeles , California , United States )
Budoff, Matthew
(
Lundquist Institute
, Torrance , California , United States )
Longenecker, Chris
(
University of Washington
, Seattle , Washington , United States )
Osoti, Alfred
(
University of Nairobi
, Nairobi , Washington , United States )
Shakil, Saate
(
University of California Los Angeles
, Los Angeles , California , United States )
Author Disclosures:
Srikanth Krishnan:DO have relevant financial relationships
;
Consultant:HeartFlow:Active (exists now)
| Matthew Budoff:DO have relevant financial relationships
;
Researcher:Lilly:Active (exists now)
; Speaker:Boehringer-Ingleheim:Active (exists now)
; Speaker:Lilly:Active (exists now)
; Speaker:Novo Nordisk:Active (exists now)
; Researcher:Novartis:Active (exists now)
; Researcher:Amgen:Active (exists now)
| Chris Longenecker:DO have relevant financial relationships
;
Advisor:Gilead Sciences:Past (completed)
| Alfred Osoti:No Answer
| Saate Shakil:DO NOT have relevant financial relationships
| ADITYA NARASHIM:No Answer
| sidney kipkorir:No Answer
| Geoffrey Omondi:No Answer
| Boni Ale:No Answer
| Bernard Gitura:No Answer
| John Kinuthia:No Answer
| Carey Farquhar:No Answer
| Priscilla Hsue:DO have relevant financial relationships
;
Consultant:Gilead:Past (completed)
; Advisor:Marea Therapeutics:Active (exists now)
; Research Funding (PI or named investigator):Abbott:Past (completed)
; Consultant:Genentech:Active (exists now)