Effectiveness of a Mobile Integrated Health vs Transitions of Care Coordinator in Heart Failure: Results from the MIGHTy-Heart Trial
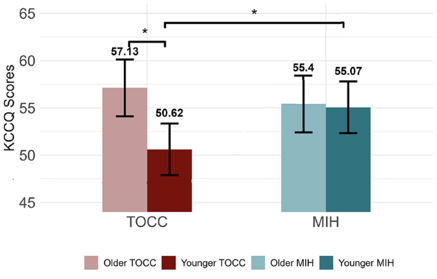
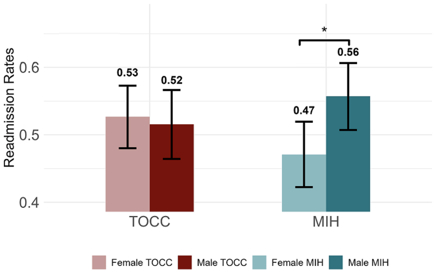
Abstract Body (Do not enter title and authors here): Background Hospital-to-home transitions are high-risk for patients with heart failure (HF). The MIGHTy-Heart pragmatic randomized clinical trial compared a Mobile Integrated Health (MIH) program with a Transitions of Care Coordinator (TOCC) intervention. MIH included a nurse care coordinator, a community paramedic home visit combined with a telehealth visit with an emergency medicine physician. TOCC involved a single nurse-led call within 48–72 hours of discharge focused on medication access, symptom review, and education. Methods A total of 2,003 patients hospitalized with HF were randomized to MIH (n=1,006) or TOCC (n=997) across 11 hospitals in New York City. Co-primary outcomes were 30-day all-cause readmissions and change in health status using the Kansas City Cardiomyopathy Questionnaire (KCCQ). Secondary outcomes included health status at 60 and 90 days and HF-specific readmissions. Analyses were conducted using intention-to-treat principles. Adjusted models, using weighted regression model to account for outcome imbalance in 30-day readmissions, controlled for age, sex, race, marital status, Elixhauser Index, and baseline KCCQ. Results Among 2,003 participants (mean age 67.6 years [SD 13.7], 52% female), 47% identified as Black or African American and 27% as Hispanic. There was no significant difference in 30-day all-cause readmission between MIH and TOCC (20.3% vs 20.4%; OR 0.99, 95% CI 0.83–1.19; p=0.95). KCCQ scores at 30 days were similar between arms (MIH: 55.6 [SD 26] vs TOCC: 53.2 [SD 25]; adjusted mean difference 1.83, 95% CI –0.75 to 4.4; p=0.16). However, subgroup analyses showed that women in the MIH arm had significantly lower odds of 30-day all-cause readmission compared to women in TOCC (OR 0.64, 95% CI 0.44–0.93; p=0.01), and patients under age 70 in the MIH arm had greater improvement in KCCQ scores at 30 days (β 4.5, 95% CI 0–8.89; p=0.05). No significant differences in readmissions were found at 60 or 90 days. Conclusion The MIGHTy-Heart trial demonstrates similar overall outcomes with both MIH and TOCC interventions to support transitions of care for hospitalized patients with heart failure. In the exploratory findings MIH supported better health status in younger patients, and women were less likely to be rehospitalized with MIH, underscoring the importance of further research to better define which patients are most likely to benefit from MIH and optimal transition of care strategies for hospitalized patients with heart failure.
Masterson Creber, Ruth
(
Columbia University
, New York , New York , United States )
Shafran Topaz, Leah
(
Weill Cornell Medical College
, New York , New York , United States )
Ellison, Melani
(
Columbia University
, New York , New York , United States )
Choi, Jacky
(
Weill Cornell Medical College
, New York , New York , United States )
Zhao, Yihong
(
Columbia University
, New York , New York , United States )
Turchioe, Meghan
(
Columbia University
, New York , New York , United States )
Daniels, Brock
(
Weill Cornell Medical College
, New York , New York , United States )
Author Disclosures:
Ruth Masterson Creber:DO NOT have relevant financial relationships
| Leah Shafran Topaz:DO NOT have relevant financial relationships
| Melani Ellison:DO NOT have relevant financial relationships
| Jacky Choi:DO NOT have relevant financial relationships
| Yihong Zhao:No Answer
| Meghan Turchioe:No Answer
| Brock Daniels:DO NOT have relevant financial relationships
Pek Pin Pin, Oh Ying Zi, Peck Kah Hua, Ong Marcus, Luo Nan, Win Phyo Thet Naing, Malhotra Rahul, Ostbye Truls, Ho Andrew Fu Wah, Lim Shir Lynn, Uy Felix Maverick Rubillar, Ho Vui Kian, Chua Jia Min