From Cardiac Emergency to Chemotherapy: Infiltrative Lymphoma Presenting With ST Elevations and Heart Failure
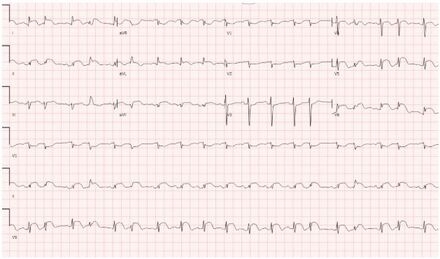
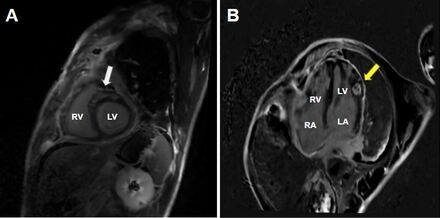
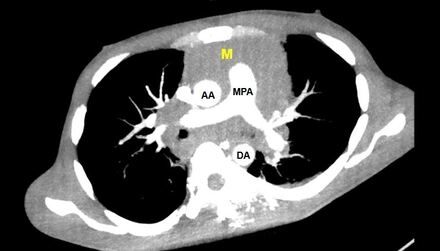
Abstract Body (Do not enter title and authors here): Case Presentation: ST-elevations on electrocardiogram are often due to cardiac emergencies such as a myocardial infarction. However, they may also signal a more occult pathology. A 35-year-old male with a past medical history of polysubstance-use disorder presented to the ED with a month-long history of chest and abdominal pain, and one day history of chest pain, orthopnea and respiratory distress. Initial vital signs significant for tachycardia to 124 bpm, otherwise normotensive, afebrile, and on room air. EKG notable for ST-elevations in the inferolateral leads. Ongoing symptoms, EKG changes, and elevated troponin prompted coronary angiography which showed no luminal disease. LVEDP was severely elevated (32 mmHg). Due to worsening respiratory distress, he was intubated and transferred to the cardiac critical care unit for suspected myocarditis. Cardiac MRI was significant for biventricular dysfunction (LVEF 30%, RVEF 32%), patchy late gadolinium enhancement (LGE) of both ventricles, and a well-circumscribed 15 mm x 15 mm region of LGE noted in the anterolateral myocardium consistent with an infiltrative mass, confirmed on CT chest imaging. Lymph node biopsy confirmed Classic Hodgkin Lymphoma. Incidentally, CT imaging of the abdomen also revealed a perforated abdominal viscous which was repaired laparoscopically. This surgery delayed systemic chemotherapy (ie high dose steroids) by 4 weeks. Patient was readmitted 3 weeks later with cardiogenic shock requiring vasopressors and intubation due to complete heart block and treated with a leadless pacemaker. Given this acute cardiac decompensation, endomyocardial biopsy was performed, revealing an aggressive B-Cell Lymphoma, thought to be a secondary primary lesion vs high-grade transformation. Patient underwent targeted radiation and multiple cycles of systemic chemotherapy, although course complicated by poor follow-up in the setting of polysubstance use and housing insecurity.
Discussion and Conclusion: As our case demonstrates, although chest pain with ST-elevations on ECG is concerning for myocardial infarction and, perhaps, even more suspicious for myocarditis in the younger adults, multimodality imaging and tissue sampling are critical in confirming the diagnosis and targeting therapy. In our case, invasive lymphoma mimicked alternative etiologies of ST elevation (namely MI and myopericarditis) and severe cardiomyopathy with notable conduction disease; tissue sampling was key to directing therapy.
Offord, Evan
(
UMass Chan Medical School
, Westborough , Massachusetts , United States )
Tai, Eric
(
UMass Chan Medical School
, Westborough , Massachusetts , United States )
Gottbrecht, Matthew
(
UMASS MEDICAL CENTER
, Worcester , Massachusetts , United States )
Author Disclosures:
Evan Offord:DO NOT have relevant financial relationships
| Eric Tai:No Answer
| Matthew Gottbrecht:No Answer