Primary Sarcomatoid Carcinoma of the Pericardium: First Reported Case and a Complex Diagnostic and Therapeutic Challenge
Abstract Body (Do not enter title and authors here): Introduction: Sarcomatoid carcinoma is an aggressive, poorly differentiated malignancy with both epithelial and mesenchymal features. While previously described in the lungs, kidneys, and soft tissues, no cases have been documented with a primary origin in the pericardium. Its diagnostic ambiguity and aggressive course present significant challenges. We present the first reported case of primary sarcomatoid carcinoma of the pericardium.
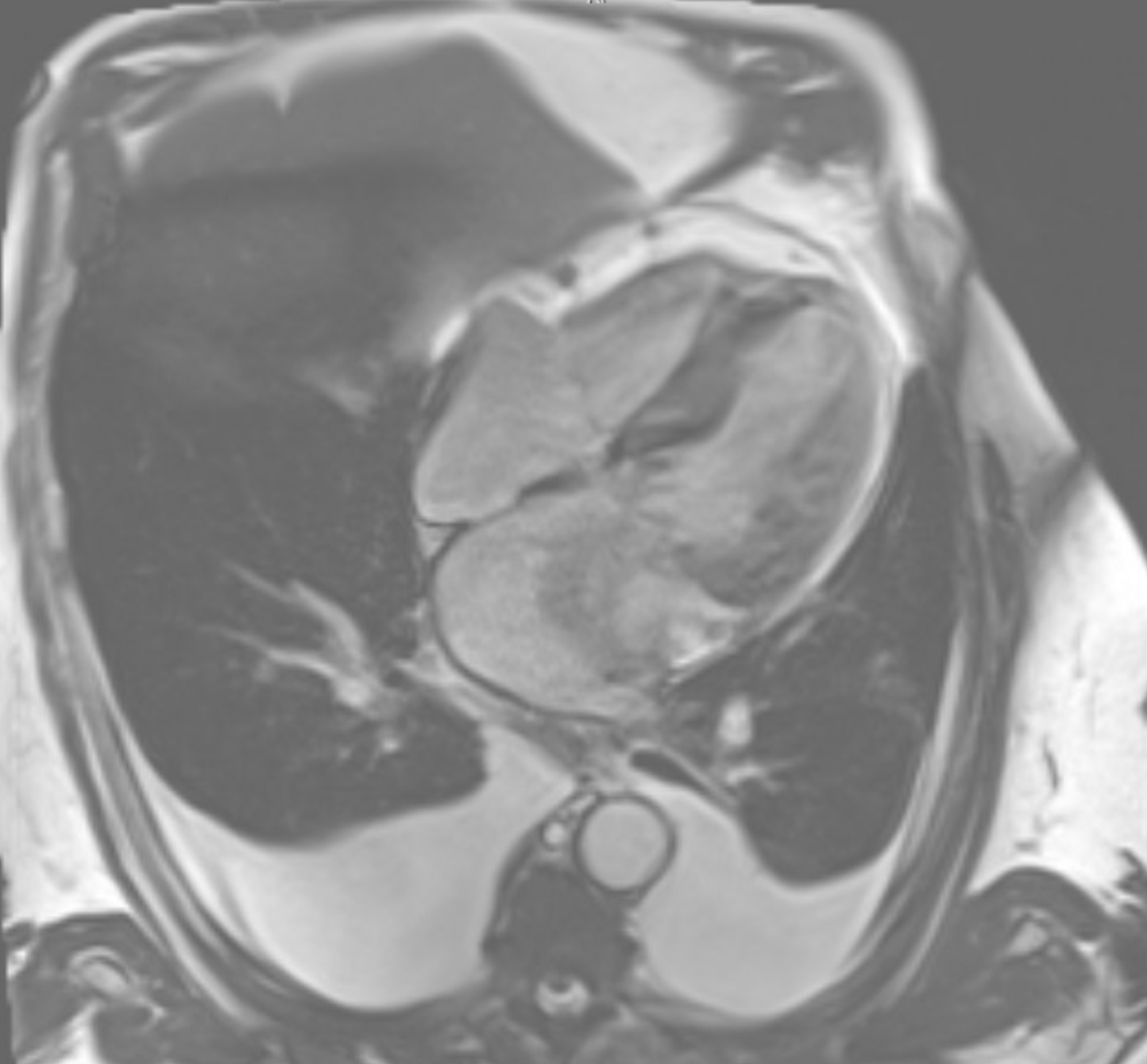
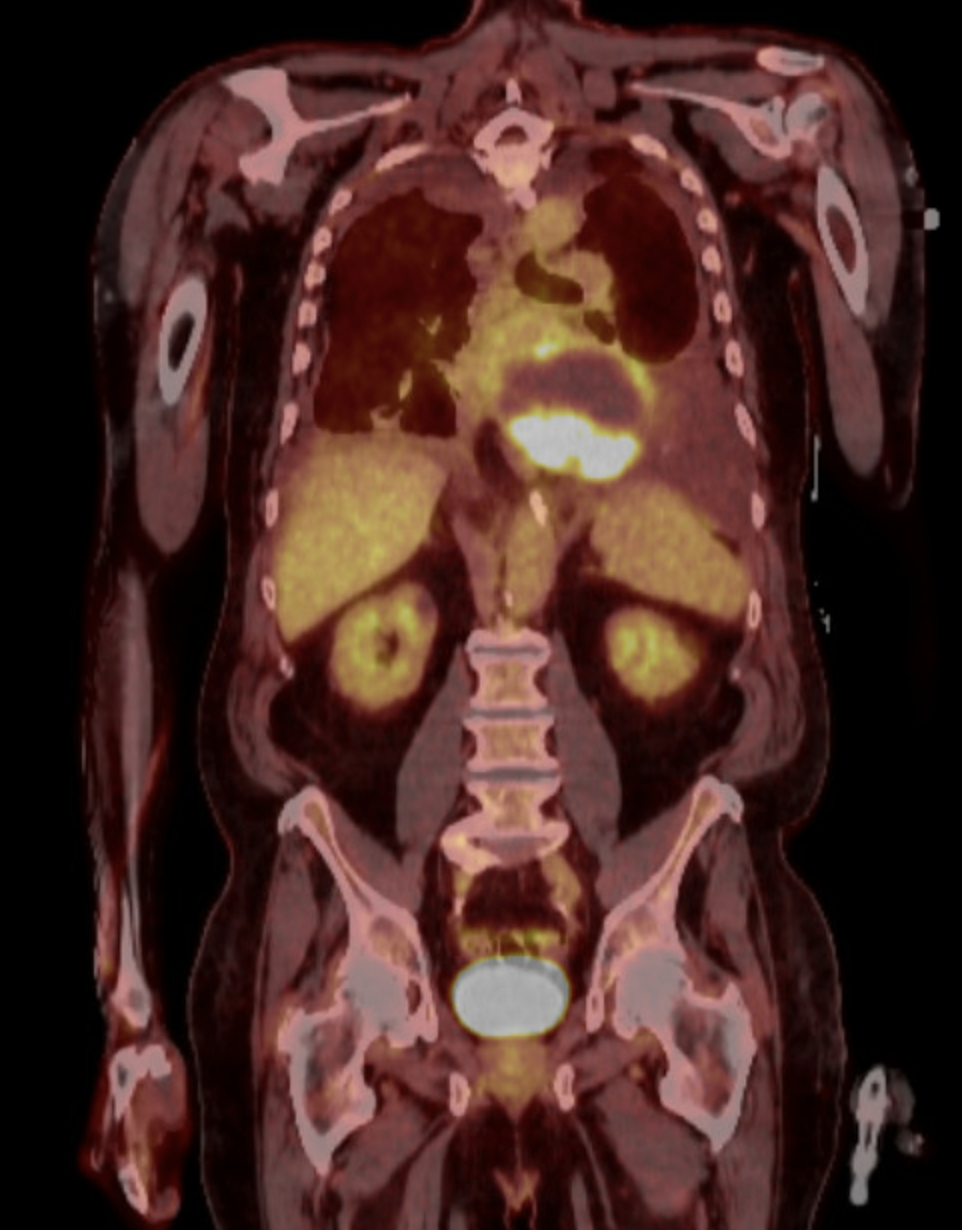
Case Description: An 81-year-old male with multiple comorbidities including hypertension, atrial fibrillation, bioprosthetic aortic valve replacement (2022), Crohn's disease, and HFmrEF presented with gastrointestinal symptoms. CT abdomen incidentally revealed a large pericardial mass (10×7 cm) compressing the left atrium and basal left ventricle, causing severe mitral stenosis (mean gradient 15 mmHg). Initial differential included mesothelioma and metastatic pulmonary sarcomatoid carcinoma. The patient underwent 10 sessions of palliative radiation. Post-radiation, he developed worsening nausea, vomiting, dysphagia, atrial fibrillation with RVR, and pleural effusions. Cardiac imaging (MRI [Figure 1] and PET [Figure 2]) confirmed the pericardial mass with compression effects and no distant metastases. Thoracentesis and supportive care provided temporary relief. Pericardial FNA pathology revealed a biphasic keratin-positive malignant neoplasm consistent with sarcomatoid carcinoma. Immunohistochemistry was positive for AE1/AE3, CK7, vimentin, and OSCAR. Negative markers ruled out mesothelioma, RCC, melanoma, and other sarcomas. Despite multidisciplinary input, the mass was inoperable. Planned AV nodal ablation and Micra pacemaker were deferred due to anesthetic risk. Inpatient chemotherapy (carboplatin + pemetrexed) was planned, but the patient decompensated before initiation.
Discussion: Sarcomatoid carcinoma of pericardial origin is undocumented. PET/CT imaging and immunohistochemistry were key to diagnosis. Tumor compression mimicked valvular and heart failure symptoms, complicating management. Despite early multidisciplinary care, prognosis was poor due to rapid clinical decline.
Conclusion: This case highlights the importance of early recognition, tissue diagnosis, and aggressive multidisciplinary planning in rare cardiac malignancies. Sarcomatoid carcinoma should be considered in the differential diagnosis of atypical pericardial masses. Further literature and registry data are needed to guide future management.
Mohammed, Adil
(
Central Michigan University
, Saginaw , Michigan , United States )
Munguti, Cyrus
(
University of Kansas Medical School
, Overland Park , Kansas , United States )
Mckinley, Grant
(
University of Kansas Medical School
, Overland Park , Kansas , United States )
Author Disclosures:
Adil Mohammed:DO NOT have relevant financial relationships
| CYRUS MUNGUTI:No Answer
| Grant McKinley:No Answer