Pulmonary Valve Endocarditis with Persistent Enterococcus Faecalis Bacteremia and Multivessel Coronary Artery Disease: A Case of Surgical Valvectomy, Coronary Bypass, and Delayed Bioprosthetic Valve Replacement
Abstract Body (Do not enter title and authors here): Background Infective endocarditis (IE) is a rare condition (15/100,000 in the US) with nonspecific symptoms, complicating diagnosis. Isolated pulmonary valve IE is exceptionally rare (1.5–2.5% of IE cases), typically linked to intravenous (IV) drug use or congenital heart disease. Enterococcus faecalis, a common IE pathogen, rarely causes isolated pulmonary valve IE. This abstract presents a rare case in a patient without typical risk factors, highlighting diagnostic and therapeutic challenges.
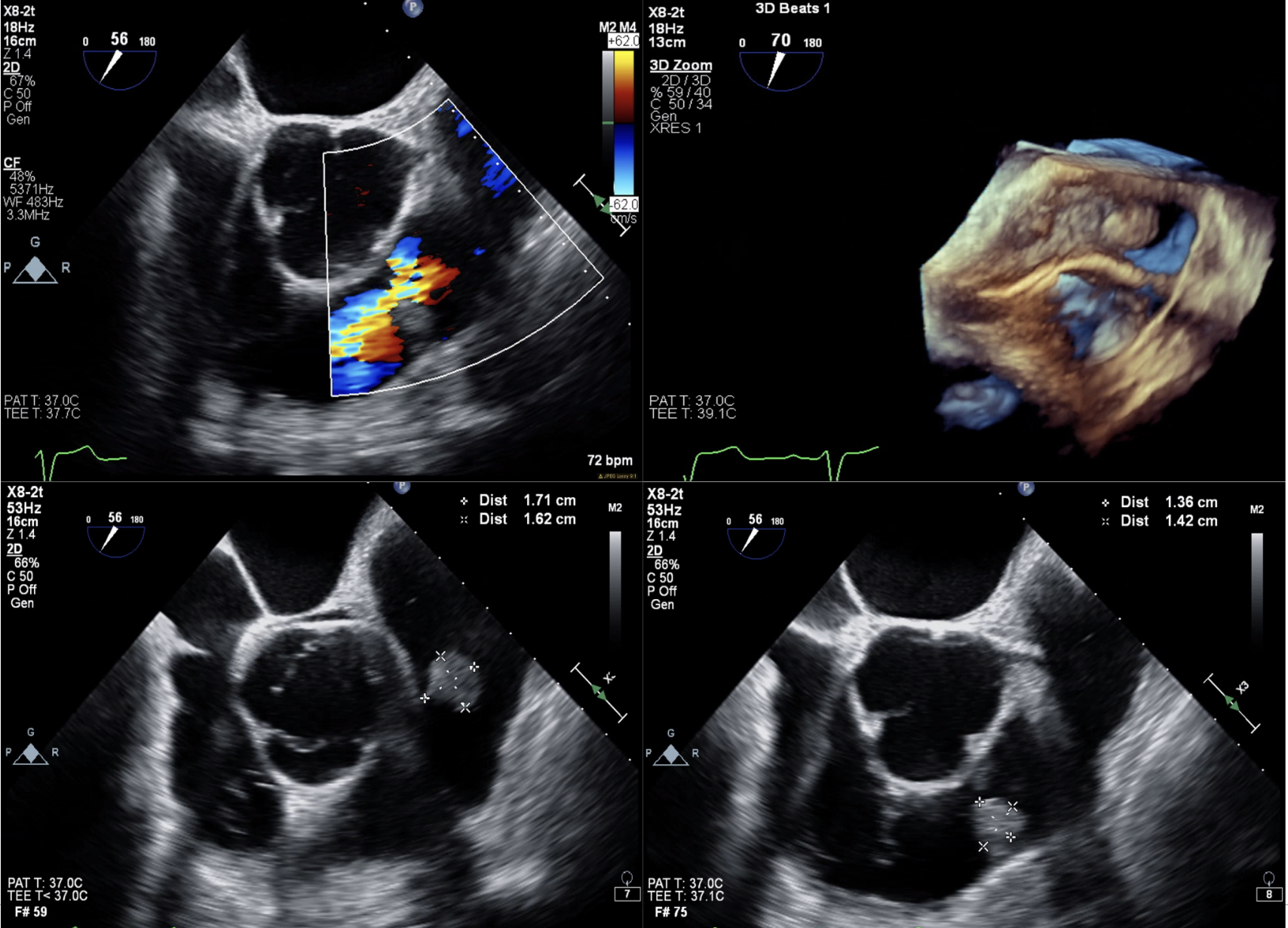
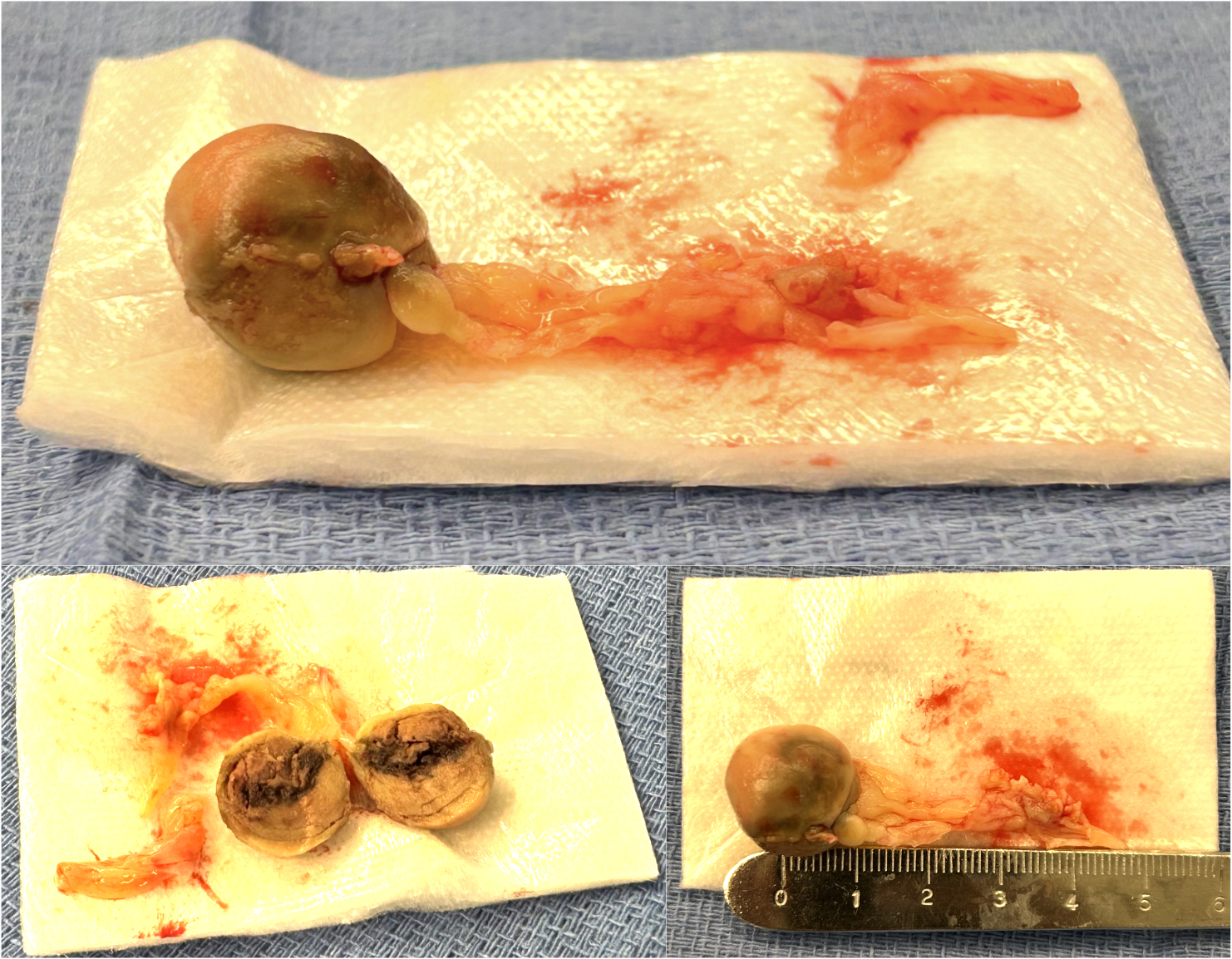
Case Description A 63-year-old male with diabetes, coronary artery disease, and recent ureteral stenting for nephrolithiasis (complicated by E. faecalis urinary tract infection) presented with malaise, chills, and polyuria. Initial evaluation revealed diabetic ketoacidosis, acute kidney injury, and E. faecalis bacteremia. Despite IV antibiotics, blood cultures remained positive for 10 days. Transesophageal echocardiogram (TEE) showed a pulmonary valve mass and moderate-to-severe regurgitation. Due to persistent infection, he underwent coronary artery bypass grafting and pulmonary valvectomy, revealing vegetations and a perforated cusp. Pathology confirmed E. faecalis endocarditis, ruling out tumors. Valve replacement was deferred due to recent bacteremia. Postoperatively, multifactorial shock required extracorporeal membrane oxygenation and mediastinal washouts for hemorrhage. Five days later, a 29-mm bioprosthetic pulmonary valve was implanted. The patient recovered and was discharged to rehabilitation.
Discussion This case highlights the challenge of diagnosing isolated pulmonary valve IE, especially with E. faecalis, given its rarity. The 2023 Modified Duke/ISCVID criteria, supported by TEE findings, confirmed IE. Persistent bacteremia necessitated surgery, consistent with complicated IE guidelines. The absence of risk factors and spheroid mass appearance initially suggested a tumor, but pathology clarified endocarditis. Right-sided IE is rare due to low pulmonary valve shear stress, making this case notable. Postoperative shock from blood loss and vasoplegia underscored the need for intensive management. Delayed valve replacement reduced reinfection risk, yielding a good outcome for this patient.
Conclusion Isolated pulmonary valve IE due to E. faecalis is rare and requires high degree of suspicion for diagnosis in persistent bacteremia. TEE, surgery, and delayed valve replacement were critical, demonstrating tailored management for favorable outcomes in complex IE.
Patel, Zeel
(
Hackensack University Medical Center
, Jersey City , New Jersey , United States )
Liu, Yang
(
Hackensack University Medical Center
, Jersey City , New Jersey , United States )
Kampaktsis, Polydoros
(
Hackensack University Medical Center
, Jersey City , New Jersey , United States )
Wengrofsky, Perry
(
Hackensack University Medical Center
, Jersey City , New Jersey , United States )
Basman, Craig
(
Hackensack University Medical Center
, Jersey City , New Jersey , United States )
Yoon, Sung-han
(
Hackensack University Medical Center
, Jersey City , New Jersey , United States )
Spallone, Rachel
(
Hackensack University Medical Center
, Hackensack , New Jersey , United States )
Author Disclosures:
Zeel Patel:DO NOT have relevant financial relationships
| Yang Liu:DO NOT have relevant financial relationships
| Polydoros Kampaktsis:No Answer
| Perry Wengrofsky:No Answer
| Craig Basman:No Answer
| Sung-Han Yoon:DO NOT have relevant financial relationships
| Rachel Spallone:No Answer