Comparison of HFpEF Cardiac Output Augmenters versus Non-Augmenters during Exercise Right Heart Catheterization
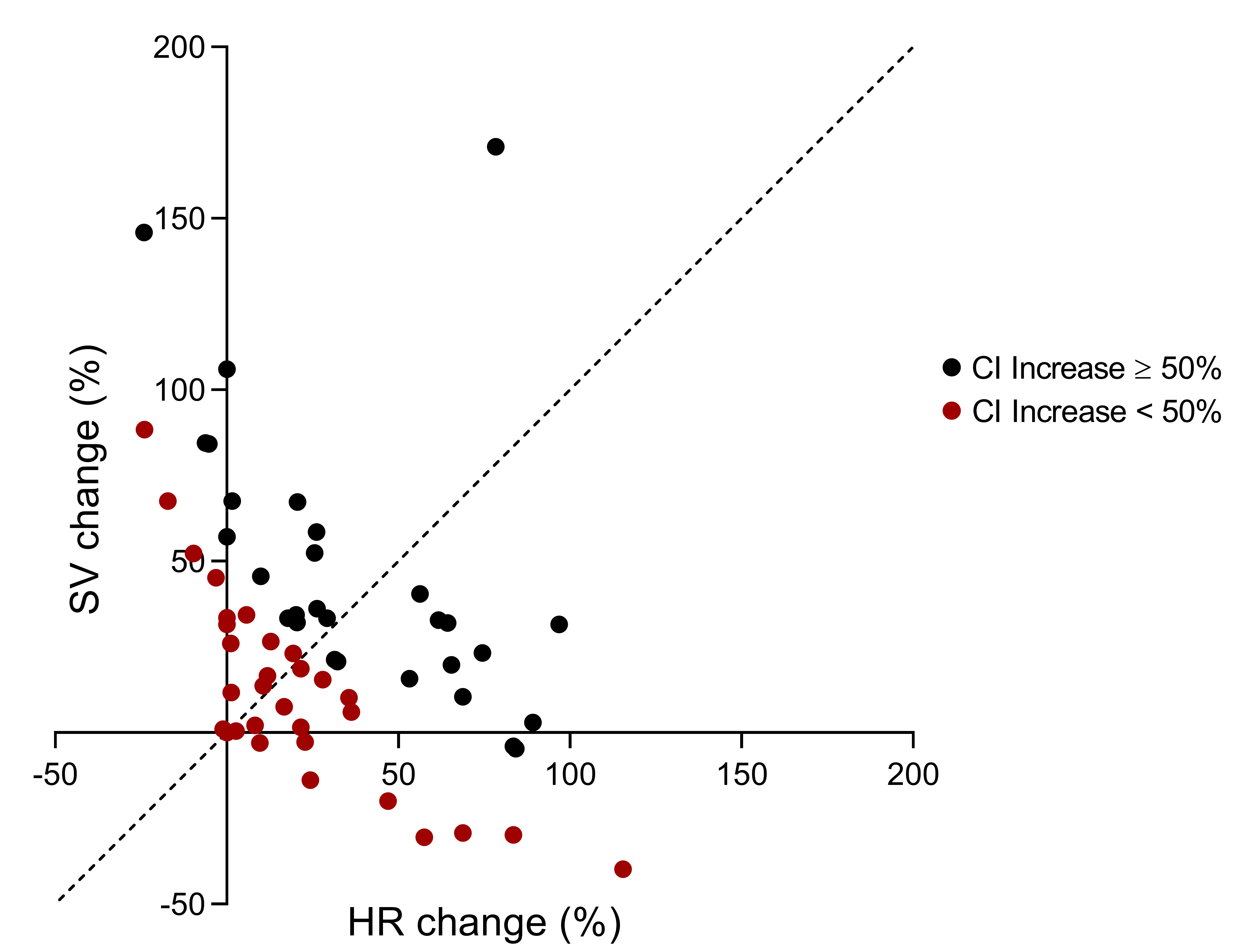
Abstract Body (Do not enter title and authors here): Introduction Exercise intolerance is a hallmark feature of heart failure with preserved ejection fraction (HFpEF), resulting in reduced quality of life. We report here several characteristics associated with a incomplete cardiac index (CI) augmentation during supine bicycle exercise RHC in patients with HFpEF. Methods We evaluated 67 patients with HFpEF and RHC exercise stress testing from the Johns Hopkins Heart Failure with Preserved Ejection Fraction Clinic. Histopathologic examination for cardiomyocyte hypertrophy, interstitial fibrosis, and inflammatory infiltrate was available 56 patients with RHC endomyocardial biopsy (EMB). Demographic, clinical, echocardiography, blood tests and pulmonary function tests (PFTs) were included in the analysis. Results We found that 60 of 67 (90%) of HFpEF patients improved their baseline CI during exercise, with a mean percent increase between baseline and maximal exercise stage of 53.5±41.6 %. The mean stage of exercise attained was 3.1±1.7 with mean energy of 26.0±17.8 watts. We further divided the patients in 2 groups: patients with ≥50% CI increase at maximal effort (HFpEF-augmenters) and, those with < 50% CI increase (HFpEF-non augmenters). HFpEF-augmenters achieved higher exercise stage, higher maximal HR and maximal SV. Of the HFpEF-augmenters, 23 (74%) saw an increase in both SV and HR; 6 (19%) increase in SV only, 2 (6%) increase in HR only. Of the HFpEF-non-augmenters, only 15 (42%) had an increase in both SV and HR, 14 (39%) had an increase in HR but decline in SV and 8 (22%) had an increase in SV but a decline in HR (Figure). Presence of comorbidities and NYHA class distribution were similar between the 2 subgroups. HFpEF-non augmenters had higher log NT-proBNP, hepatic enzymes, uric acid and cystatin C, lower cholesterol, higher pulmonary vascular resistance and lower PFTs (total lung capacity, forced vital capacity and FEV1) than HFpEF-augmenters (Table). Degrees of hypertrophy, fibrosis and inflammation on EMB did not differ between groups. Conclusion In an obese HFpEF cohort with exercise hemodynamic testing those unable to augment cardiac index had a variable degree of chronotropic and inotropic/lusitropic incompetence, higher log NT-proBNP, elevated markers of hepatic and renal impairment, lower cholesterol and lower PFTs.
Tanacli, Radu
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Tajdini, Masih
(
Johns Hopkins University School of
, Baltimore , Maryland , United States )
Jani, Vivek
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Hahn, Virginia
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Sharma, Kavita
(
Johns Hopkins University SOM
, Baltimore , Maryland , United States )
Author Disclosures:
Radu Tanacli:DO NOT have relevant financial relationships
| Masih Tajdini:DO NOT have relevant financial relationships
| Vivek Jani:DO NOT have relevant financial relationships
| Virginia Hahn:DO NOT have relevant financial relationships
| Kavita Sharma:DO have relevant financial relationships
;
Consultant:Alleviant:Active (exists now)
; Consultant:Eli Lily:Active (exists now)
; Consultant:Rivus:Active (exists now)
; Consultant:NovoNordisk:Active (exists now)
; Consultant:Novartis:Active (exists now)
; Consultant:Edwards LifeSciences:Active (exists now)
; Consultant:AstraZeneca:Active (exists now)
; Consultant:Bayer:Active (exists now)