Health System Variability in Lipid Management for Patients with Atherosclerotic Cardiovascular Disease: An Analysis from Cv-MOBIUS
Abstract Body (Do not enter title and authors here): Background: Nationally, many ASCVD patients fail to achieve an LDL-C <70 mg/dL, and uptake of both statin and non-statin therapies is low. The degree to which this varies across health systems is less clear.
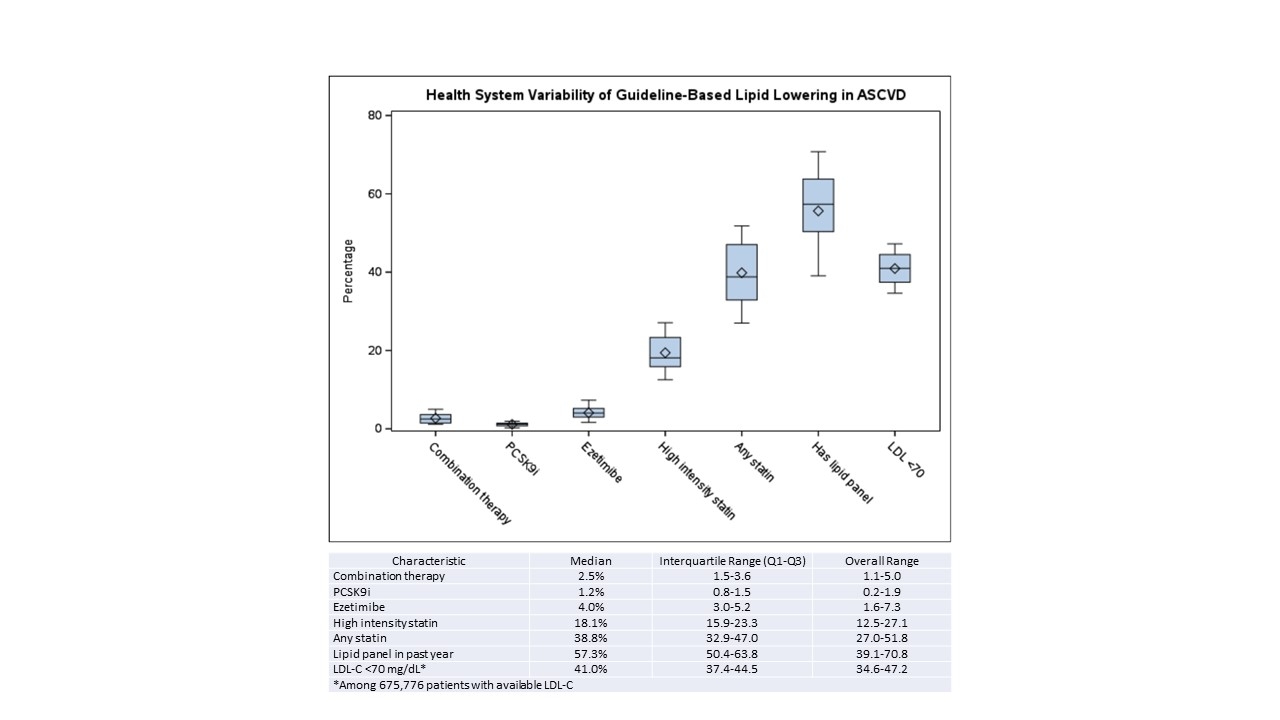
Methods: A cross sectional analysis was performed where lipid levels and lipid lowering therapies (LLT) were assessed using electronic health record data in patients with a previous diagnosis of ASCVD. The data was obtained across 14 US healthcare systems between 1/1/2021-12/31/2022. Proportions of patients with an active prescription of any statin, high intensity statin, ezetimibe, PCSK9i, and combination therapy (two or more agents) within 395 days of the most recent LDL-C value (index date) was evaluated overall and by participating site. Additionally, the proportion of patients with an LDL-C <70 mg/dL at the index date was also assessed.
Results: Across 14 health systems, 1,118,623 patients with ASCVD were identified (median 61,840 per health system, range 8,161-182,315). Overall, 675,776 (60.4%) had an LDL-C level in the past year (range 39.1% - 70.8%). Of those with a lipid level, achievement of LDL-C <70 mg/dL ranged from 34.6-47.2%. In total, 42.6% were on any statin, 20.1% were on a high intensity statin, 4.3% on ezetimibe, and 1.2% on a PCSK9i. Only 2.9% were on combination therapy of a statin with ezetimibe or a PCSK9i. Variability was seen across health systems in utilization of each of these therapies, however even in the highest performing health systems, LLT uptake and achievement of LDL-C < 70mg/dL remained low (Figure).
Conclusion: Variability in utilization of LLT in ASCVD patients between health systems suggests that system-level factors may impact achieving guideline-based LDL-C goals. Despite the variability, the highest proportion of patients achieving an LDL-C <70mg/dL remained under 50% indicating the need for aggressive implementation efforts.
Shah, Nishant
(
Duke University Medical Center
, Durham , North Carolina , United States )
Shrader, Peter
(
Duke University Medical Center
, Durham , North Carolina , United States )
Shoji, Satoshi
(
Keio University School of Medicine
, Shinjyuku, Tokyo , Japan )
Martin, Seth
(
Johns Hopkins School of Medicine
, Baltimore , Maryland , United States )
Fernandez, Soledad
(
The Ohio State University
, Columbus , Ohio , United States )
Chamberlain, Alanna
(
MAYO CLINIC
, Rochester , Minnesota , United States )
Arnold, Jonathan
(
University of Pittsburgh, UPMC
, McKeesport , Pennsylvania , United States )
Shapiro, Michael
(
Wake Forest Univ School of Medicine
, Winston Salem , North Carolina , United States )
Effron, Mark
(
OCHSNER MEDICAL CENTER
, New Orleans , Louisiana , United States )
Chrischilles, Elizabeth
(
University of Iowa
, Iowa City , Iowa , United States )
Allred, Clint
(
St Luke's Health System
, Meridian , Idaho , United States )
Priest, Elisa
(
Baylor Scott & White Research Institute
, Dallas , Texas , United States )
Syed, Mahanazuddin
(
UTHSCSA
, San Antonio , Texas , United States )
Kirchner, H Lester
(
Geisinger
, Danville , Pennsylvania , United States )
Leja, Monika
(
University Of Michigan
, Ann Arbor , Michigan , United States )
Ahmad, Zahid
(
UT SOUTHWESTERN MEDICAL CENTER
, Dallas , Texas , United States )
Kalich, Bethany
(
Amgen
, San Antonio , Texas , United States )
Shoji Satoshi, Jones Laney, Peterson Eric, Navar Ann Marie, Shah Nishant, Shrader Peter, Freeman Nikki, Bittner Vera, Wilcox Tanya, Amanda C Doran, Wojcik Cezary, Jin Ran