Immediate versus staged percutaneous coronary intervention of non-culprit lesions in patients with st-elevation myocardial infarction and multivessel disease: a meta-analysis of 4,120 patients.
Abstract Body (Do not enter title and authors here): Introduction Multivessel coronary artery disease is common in patients with ST-segment elevation myocardial infarction (STEMI). Previous trials have shown that comprehensive revascularization of non-culprit arteries with significant stenosis reduces the risks of cardiovascular death, myocardial infarction, and ischemia-driven revascularization compared to culprit-only revascularization. However, the optimal timing for revascularizing non-culprit lesions—immediate versus staged percutaneous coronary intervention (PCI)—remains unclear. This meta-analysis aims to determine if staged or immediate PCI is associated with fewer major adverse cardiovascular events.
Methods A meta-analysis was conducted following PRISMA guidelines, with a protocol registered in PROSPERO (CRD42023485163). We included studies from PubMed, Embase, and Cochrane databases until October 10, 2023. Inclusion criteria were: 1) patients over 18 with STEMI and hemodynamically stable multivessel disease; 2) intervention: immediate PCI; 3) comparator: staged PCI; 4) study types: randomized clinical trials (RCTs) and cohort studies. Study quality was assessed using ROBINS-I for observational studies and ROB 2 for RCTs.
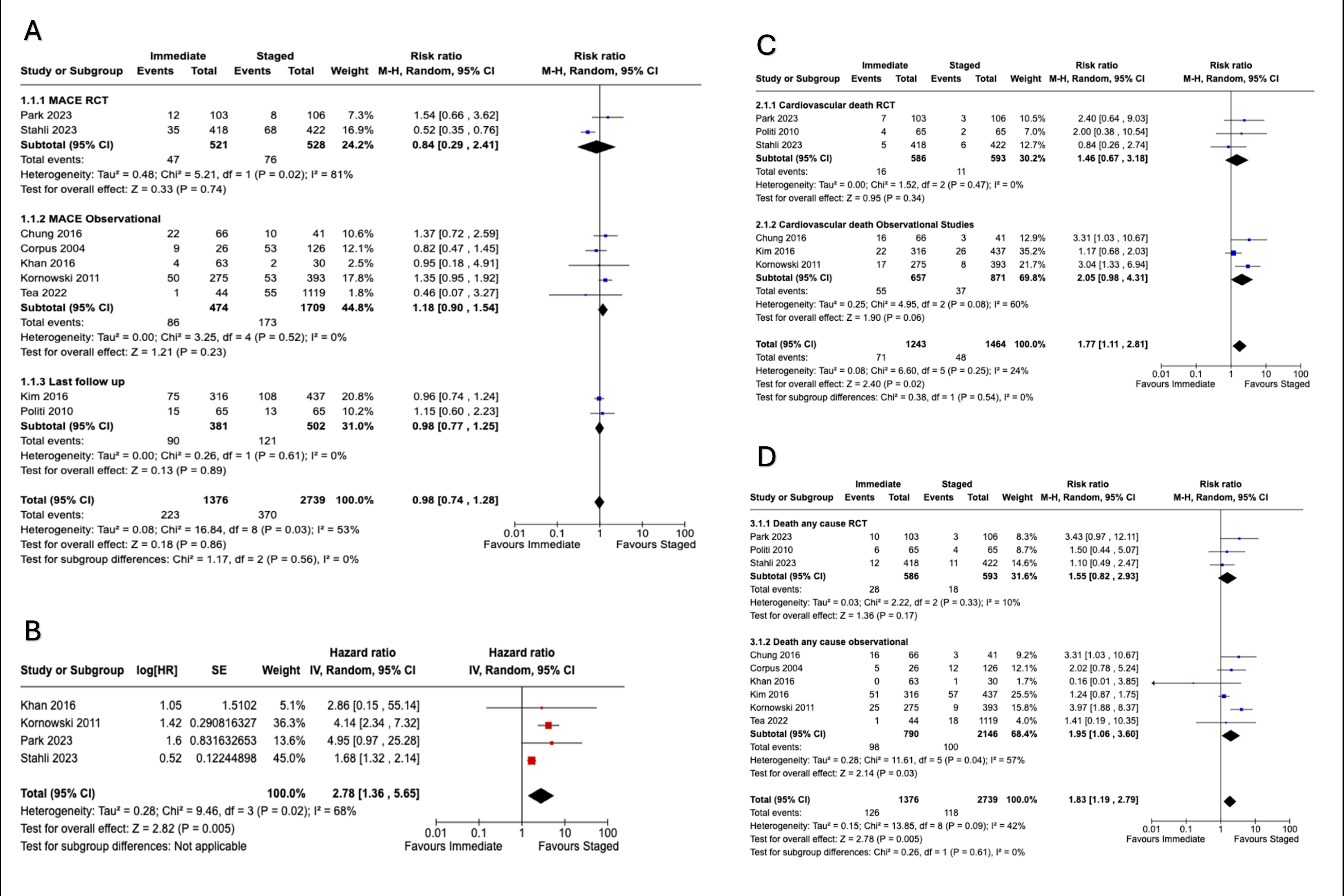
Results Nine studies met inclusion criteria: 3 RCTs and 6 cohort studies, with a total of 4,120 patients. Staged PCI was significantly associated with reduced cardiovascular death (RR = 1.77; 95% CI = 1.11-2.81; p = 0.02, I2 = 24%) and all-cause mortality (RR = 1.83; 95% CI = 1.19-2.79; p = 0.005, I2 = 42%). Hazard ratio analysis also favored staged PCI for cardiovascular death (HR = 4.11; 95% CI = 1.07-5.87; p = 0.04, I2 = 12%) and all-cause mortality (HR = 8.13; 95% CI = 1.01-8.17; p = 0.05, I2 = 37%). No significant differences were found for major adverse cardiovascular events (RR = 0.98; 95% CI = 0.74-1.28; p = 0.86, I2 = 53%) or in major bleeding, stroke, or target vessel revascularization.
Conclusion In patients with STEMI and multivessel disease, staged coronary revascularization is associated with a lower risk of major adverse cardiovascular events, cardiovascular death, and all-cause mortality compared to immediate revascularization, without increasing adverse outcomes. Further research is needed to confirm these findings.
Paulino, Daniel
(
Universidad Autonoma Metropolitana
, Mexico City , Mexico City , Mexico )
Andrade Arbaiza, Edwin
(
Universidad de El Salvador
, San Miguel , San Miguel , El Salvador )
Navarro Martinez, Daniel
(
Indiana University
, Indianapolis , Indiana , United States )
Xiloj, Shirley
(
Universidad de San Carlos de Guatemala
, Guatemala , Guatemala , Guatemala )
Hernandez, Bruno
(
Universidad Nacional Autónoma de México
, Mexico City , Mexico City , Mexico )
Garcia-mena, Lissette
(
Universidad Nacional Autónoma de México
, Mexico City , Mexico City , Mexico )
Author Disclosures:
Daniel Paulino:DO NOT have relevant financial relationships
| Edwin Andrade Arbaiza:DO NOT have relevant financial relationships
| Daniel Navarro Martinez:DO NOT have relevant financial relationships
| Shirley Xiloj:DO NOT have relevant financial relationships
| Bruno Hernandez:DO NOT have relevant financial relationships
| Lissette Garcia-Mena:DO NOT have relevant financial relationships