Higher Intraoperative Blood Pressure Targets Are Associated with Reduced Delirium After Cardiac Surgery
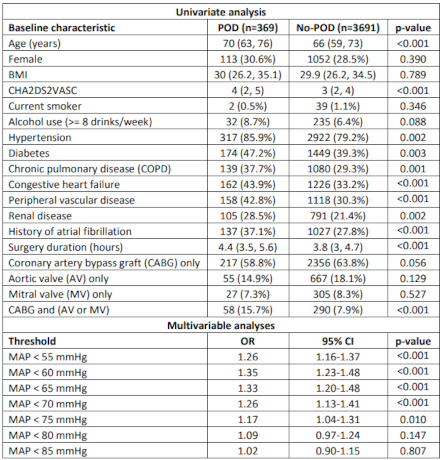
Abstract Body (Do not enter title and authors here): Background: Intraoperative hypotension has been associated with several adverse outcomes including postoperative delirium (POD). While current guidelines recommend an intraoperative mean arterial pressure (MAP) above 65 mmHg during non-cardiac operations, there is no clear consensus regarding the optimal MAP threshold for cardiac surgery patients. We aim to determine an intraoperative MAP threshold that is associated with a reduced risk of delirium following cardiac surgery. Methods: We established a retrospective observational cohort of adult patients who underwent cardiac surgery within our healthcare system between 2014 and 2021. After excluding patients with preoperative delirium or with no documented Confusion Assessment Method for the ICU (CAM-ICU) result, the final cohort included 4,060 patients. Delirium was defined as a positive CAM-ICU test in a patient with a Richmond Agitation-Sedation Scale (RASS) >= -3. Intraoperative hypotension was defined as the number of MAP measurements below a threshold, k, normalized by the total number of MAP measurements. We experimented with k = 55, 60, 65, …, and 85 mmHg. Separate multivariable logistic regression analyses were conducted for each threshold, k, to investigate its association with POD. Results: POD was documented in 369 patients (9.1%). Patients with POD had higher median age (70 vs 66 years, p<0.001), CHA2DS2VASC score (4 vs 3, p<0.001), and surgery duration time (4.4 vs 3.8 hours, p<0.001). Multivariable regression analysis, summarized in Table 1, showed that intraoperative MAP values below 75 mmHg were consistently associated with increased risk for POD. The number of drops in intraoperative MAP measurements below 75 mmHg was associated with higher risk of POD (adjusted OR=2.17, p=0.010), while the number of drops in intraoperative MAP measurements below 80 mmHg was not significantly associated with higher risk of POD (adjusted OR=1.65, p=0.147). Conclusions: Our results suggest that using a threshold of 75 mmHg for intraoperative MAP during cardiac operations may reduce the incidence of POD. Further research, including prospective clinical studies, is needed to validate and ensure the generalizability of our findings across diverse patient populations.
Abbas, Mostafa
(
Geisinger
, Danville , Pennsylvania , United States )
Morland, Thomas
(
Geisinger
, Danville , Pennsylvania , United States )
Sharma, Rohit
(
Geisinger
, Danville , Pennsylvania , United States )
Kirchner, H Lester
(
Geisinger
, Danville , Pennsylvania , United States )
Lemaire, Scott
(
Geisinger
, Danville , Pennsylvania , United States )
El-manzalawy, Yasser
(
Geisinger
, Danville , Pennsylvania , United States )
Author Disclosures:
Mostafa Abbas:No Answer
| Thomas Morland:No Answer
| ROHIT SHARMA:DO NOT have relevant financial relationships
| H Lester Kirchner:DO NOT have relevant financial relationships
| Scott LeMaire:No Answer
| Yasser El-Manzalawy:DO NOT have relevant financial relationships