Scientific Sessions 2024
/
New Directions in Heart Failure
/
Difference of escalation and de-escalation strategies and outcome in cardiogenic shock patients supported with Impella; acute myocardial infarction versus de novo heart failure versus acute on chronic heart failure
American Heart Association
172
0
Final ID: Su2147
Difference of escalation and de-escalation strategies and outcome in cardiogenic shock patients supported with Impella; acute myocardial infarction versus de novo heart failure versus acute on chronic heart failure
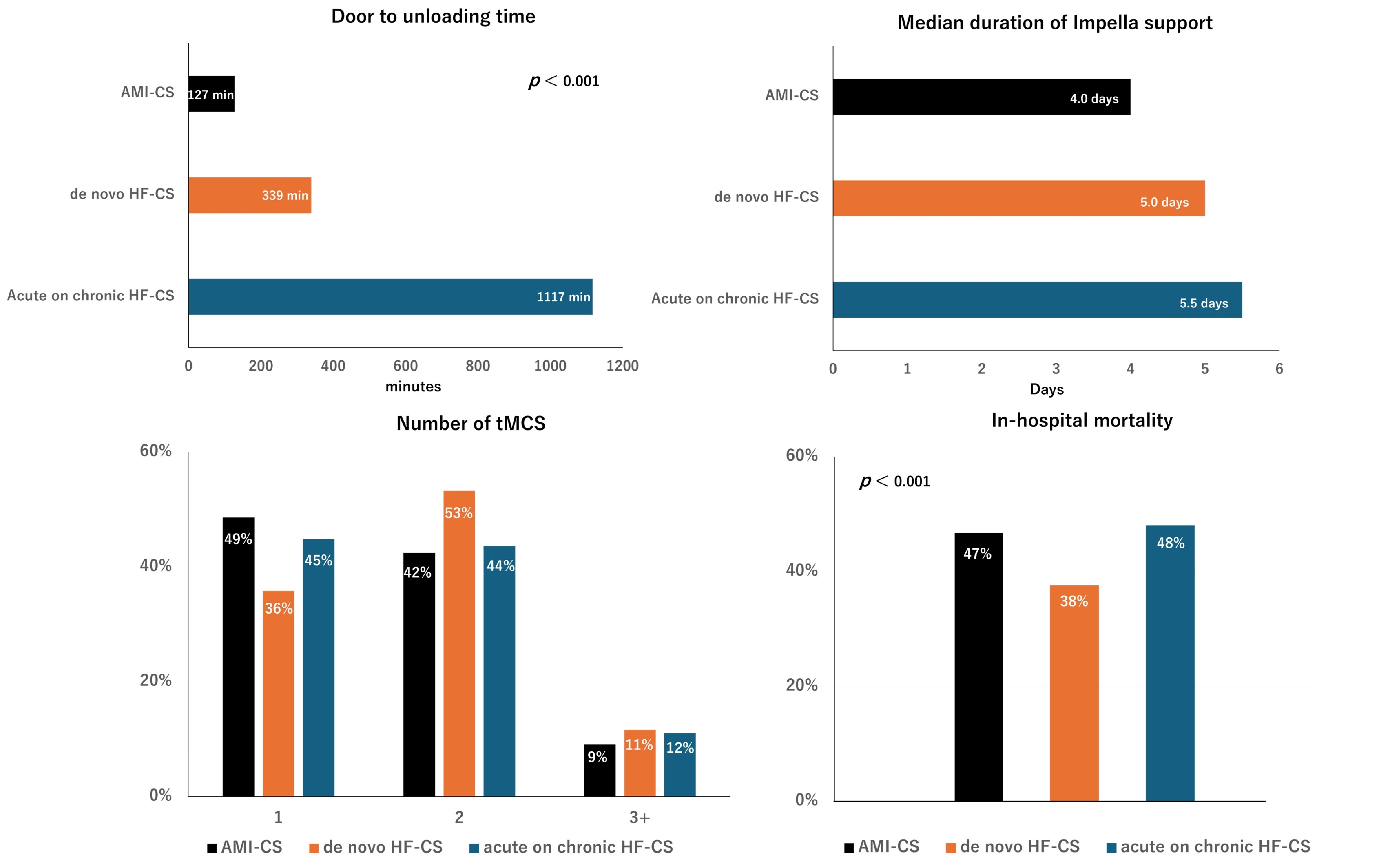
Abstract Body (Do not enter title and authors here): Background: Timely initiation of temporary mechanical circulatory support (tMCS), escalation and de-escalation strategies are key components for treatment of cardiogenic shock (CS). However, little is known about tMCS strategies and outcomes based on etiology of CS and chronicity of heart failure. We evaluated differences of tMCS strategies and outcome in patients supported with Impella in acute myocardial infarction related CS (AMI-CS), de novo heart failure related CS (de novo HF-CS), and acute on chronic heart failure related CS (acute on chronic HF-CS). Methods and Results: The Japan Registry for Percutaneous Ventricular Assist Device (J-PVAD) is multicenter, observational registry enrolling all consecutive patients treated with Impella in Japan. We conducted a retrospective analysis of patients with Impella in J-PVAD between February 2020 and December 2022. Among 3678 CS patients supported with Impella. 2418 (65.7%) patients were presented with AMI-CS, 758 (20.6%) patients with de novo HF-CS, and 502 (13.7%) patients with acute on chronic HF-CS. The median time from hospital entry to initiation of Impella were 127 min, 339 min, and 1117 min in AMI-CS, de novo HF-CS, and acute on chronic HF-CS, respectively (P < 0.001 for each). 2233 (92.4%) patients with AMI-CS underwent percutaneous coronary intervention during index hospitalization with median door-balloon-time of 108 min. Patients treated with multiple mechanical circulatory supports were 51.4%, 64.2%, and 55.2% in AMI-CS, de novo HF-CS, and acute on chronic HF-CS, respectively. Using de novo CS-HF as a reference, the risk for in-hospital mortality for AMI-CS and acute on chronic HF-CS were: odds ratio (OR) 1.24 [95% confidence interval (CI) 1.04–1.50], P = 0.02 and OR 1.43 (95% CI 1.12–1.81), P = 0.004, respectively. Conclusions In CS patients supported with Impella, time course and utilization of tMCS varied in AMI-CS, de novo HF-CS, and acute on chronic HF-CS. De novo HF-CS had significantly better mortality relative to AMI-CS and acute-on-chronic CS. Further research is required for tMCS strategies based on etiology of CS and chronicity of heart failure.
Hattori, Hidetoshi
(
Tokyo women's medical university
, Tokyo , Japan )
Kikuchi, Noriko
(
Tokyo women's medical university
, Tokyo , Japan )
Ichihara, Yuki
(
Tokyo women's medical university
, Tokyo , Japan )
Saito, Satoshi
(
Tokyo women's medical university
, Tokyo , Japan )
Nunoda, Shinichi
(
Tokyo Women's Medical University Graduate School of Medicine
, Tokyo , Japan )
Niinami, Hiroshi
(
Tokyo women's medical university
, Tokyo , Japan )
Yamaguchi, Junichi
(
Tokyo women's medical university
, Tokyo , Japan )
., J-pvad Investigators
(
None
, Tokyo , Japan )
Author Disclosures:
Hidetoshi Hattori:DO NOT have relevant financial relationships
| Noriko Kikuchi:DO NOT have relevant financial relationships
| Yuki Ichihara:DO NOT have relevant financial relationships
| Satoshi Saito:DO NOT have relevant financial relationships
| Shinichi Nunoda:No Answer
| Hiroshi Niinami:DO NOT have relevant financial relationships
| Junichi Yamaguchi:No Answer
| J-PVAD investigators .:No Answer