Looking Beyond Respirophasic Ventricular Interdependence: A Case Report of Constrictive Pericarditis Masquerading as Cirrhosis
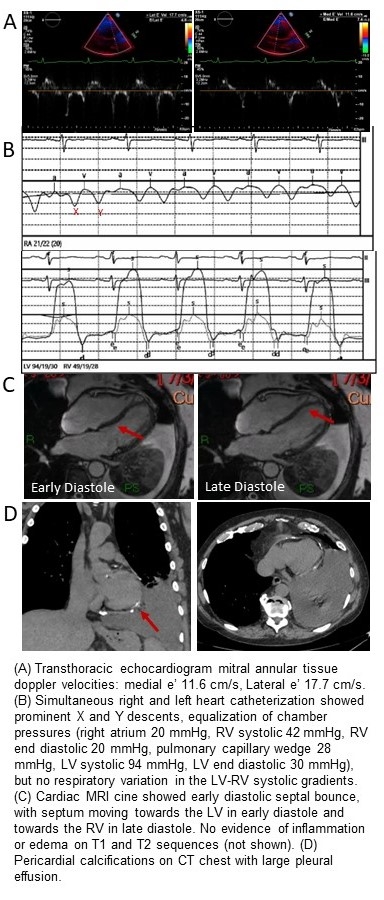
Abstract Body (Do not enter title and authors here): Case Presentation A 67-year-old man with recurrent pleural effusions and concern for cirrhosis was referred for liver transplant. Pleural fluid was transudative by Light’s criteria with a high total protein level of 3.5 g/dL, which made hepatic hydrothorax unlikely. Liver biopsy confirmed congestive hepatopathy without advanced fibrosis. Transthoracic echocardiogram showed left ventricular (LV) ejection fraction 55%, right ventricular (RV) systolic pressure 35 mmHg, normal mitral annular tissue doppler velocities, and early diastolic septal bounce. Right and left heart catheterization showed prominent X and Y descent, elevated and equalized diastolic pressures, but no respiratory discordance in the LV-RV pressure gradient. As etiology of these findings were unclear, he underwent aggressive diuresis and hemodialysis, but repeat right heart catheterization showed persistently elevated right and left filling pressures. Cardiac MRI had no evidence of myocardial or pericardial inflammation/edema but showed pericardial thickening (7.9 mm) and septal bounce. There was no inspiratory septal shift, but the large pleural effusion appeared to limit diaphragm excursion. Given lack of respirophasic ventricular interdependence and thickened pericardium on MRI, CT was ordered, showing pericardial calcifications. Diagnosis of constrictive pericarditis was made, and patient underwent complete pericardiectomy. Pathology confirmed calcified and thick pericardium without acute inflammation. Post-operatively, patient developed RV failure, but recovered with inotrope support and was discharged with improvement in congestive symptoms.
Discussion Constrictive pericarditis classically exhibits respirophasic ventricular interdependence, but large pleural effusions may decrease respiratory variation in intrathoracic pressures, blunting this response. Normal mitral annulus tissue doppler velocities and lack of infiltrative process on cardiac MRI made restrictive cardiomyopathy unlikely. In the absence of respirophasic changes on multimodality testing, constriction can be diagnosed with other supportive features such as diastolic septal bounce, rapid Y descent, diastolic pressure equalization, and pericardial thickening and calcifications.
Shan, Rongzi
(
Cedars Sinai Medical Center
, Los Angeles , California , United States )
Share, Michael
(
Cedars Sinai Medical Center
, Los Angeles , California , United States )
Ayoub, Walid
(
Cedars Sinai Medical Center
, Los Angeles , California , United States )
Lee, Andrew
(
Cedars Sinai Medical Center
, Los Angeles , California , United States )
Kwan, Alan
(
Cedars Sinai Medical Center
, Los Angeles , California , United States )
Author Disclosures:
Rongzi Shan:DO NOT have relevant financial relationships
| Michael Share:No Answer
| Walid Ayoub:DO NOT have relevant financial relationships
| Andrew Lee:No Answer
| Alan Kwan:DO have relevant financial relationships
;
Consultant:InVision Technology Corporation:Active (exists now)