Feasibility and Implications of Electrocardiogram-based Prediction of Incessant Refractory Ventricular Fibrillation
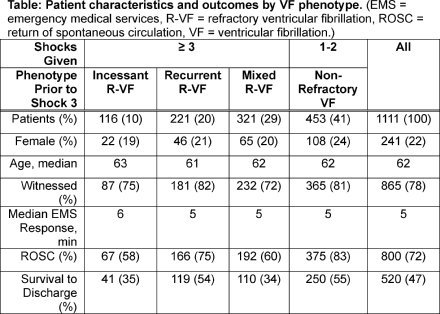
Abstract Body: Background Refractory ventricular fibrillation (R-VF) patients, defined as requiring ≥ 3 shocks during resuscitation of OHCA, have relatively poor outcomes. Prior studies have predicted R-VF using the ECG, suggesting potential to guide early patient-specific treatment for R-VF. However, R-VF comprises multiple phenotypes with distinct defibrillation response profiles: Incessant VF (no shocks terminate VF), recurrent VF (all shocks terminate VF but VF recurs), or mixed VF (shocks variably terminate VF). These phenotypes may have distinct prognoses, and may also respond differently to R-VF treatments such as early antiarrhythmics, modified vasopressor dosing, alternative defibrillation strategies, or expedited invasive interventions. Early prediction of specific R-VF phenotype could potentially improve outcome through preemptive targeting of treatment to individual phenotype. Aim We sought to predict incessant R-VF using machine learning analysis of the defibrillator ECG. Methods We performed a retrospective study of adult VF OHCA treated by EMS from 2006–2019 in King County WA. We linked a clinical OHCA registry with defibrillator recordings to evaluate ROSC and survival to hospital discharge by VF type (non-refractory; or incessant, recurrent, or mixed R-VF prior to the third shock). To predict incessant R-VF specifically, we used a series of four 2-s ECG segments from each patient within 60s surrounding the first shock. Patients were randomized 65%/35% for training/test. A support vector machine classifier was trained to predict subsequent incessant R-VF using ECG scalograms. Algorithm performance was assessed by area under the receiver operating characteristic curve (AUC) and by sensitivity at >75% specificity. Results Of 1111 included VF patients, median age was 62, 241 (22%) were female, 658 (59%) were refractory (≥ 3 shocks), 800 (72%) achieved ROSC, and 520 (47%) survived. The incessant R-VF phenotype accounted for 10% (N=116) and had worse ROSC and survival compared to recurrent R-VF and non-refractory patients (Table). Training and test AUCs to predict incessant R-VF were 0.77 (95% CI: 0.72–0.82, N=723) and 0.76 (95% CI: 0.66–0.82, N=388) respectively. Test sensitivity and specificity were 64% and 76%. Conclusion Refractory VF comprises distinct phenotypes with disparate outcomes. Incessant R-VF has notably poor prognosis. Machine learning may be able to predict incessant R-VF, potentially guiding preemptive, patient-specific treatments to improve outcome.
Coult, Jason
(
University of Washington
, Seattle , Washington , United States )
King, Julia
(
University of Washington
, Seattle , Washington , United States )
Kwok, Heemun
(
UNIVERSITY OF WASHINGTON
, Seattle , Washington , United States )
Bhandari, Shiv
(
University of Washington
, Seattle , Washington , United States )
Blackwood, Jennifer
(
KING COUNTY EMS
, Seattle , Washington , United States )
Johnson, Nicholas
(
University of Washington
, Seattle , Washington , United States )
Sayre, Michael
(
, Seattle , Washington , United States )
Daya, Mohamud
(
OHSU
, Portland , Oregon , United States )
Rea, Thomas
(
University of Washington
, Seattle , Washington , United States )
Kudenchuk, Peter
(
University of Washington
, Seattle , Washington , United States )
Author Disclosures:
Jason Coult:DO NOT have relevant financial relationships
| Peter Kudenchuk:No Answer
| Julia King:DO NOT have relevant financial relationships
| Heemun Kwok:No Answer
| Shiv Bhandari:DO NOT have relevant financial relationships
| Jennifer Blackwood:DO NOT have relevant financial relationships
| Nicholas Johnson:DO have relevant financial relationships
;
Advisor:Neuroptics, Inc:Active (exists now)
| Michael Sayre:DO have relevant financial relationships
;
Consultant:Stryker Emergency Response:Past (completed)
| Mohamud Daya:DO NOT have relevant financial relationships
| Thomas Rea:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Philips:Active (exists now)
; Advisor:Resuscitation Academy Foundation:Active (exists now)
; Research Funding (PI or named investigator):NIH:Active (exists now)
; Research Funding (PI or named investigator):Stryker:Active (exists now)
Bueno Claudia, Souza Barbara, Santos Aline, Da Silva Ferreira Laíse Jorrana, Varao Thawanny, Cunha Carneiro Maria Angelica, Gomes Laysa, Teixeira Costa Ana Carolina, Miranda Luana, Martin Joelma, Rocha Nathalia, Dias Adria