A Contactless and Automated Approach to the Acute Stroke Assessment
Abstract Body: Objectives: Acute stroke assessments occur in various settings, such as homes, ambulances, emergency rooms, and hospitals. The standard assessment is an in-person evaluation by healthcare providers using the National Institutes of Health Stroke Scale (NIHSS). This study aims to assess the accuracy of a contactless, automated method for estimating the duration of various NIHSS neurological tests.
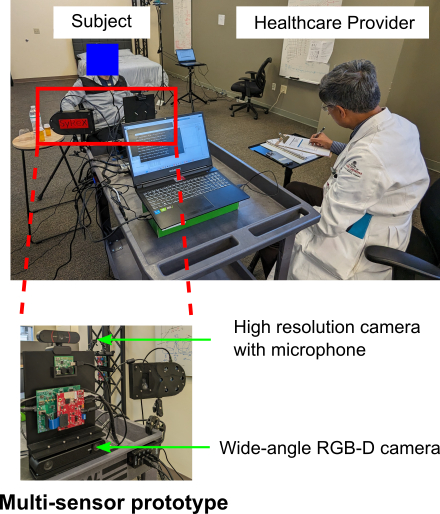
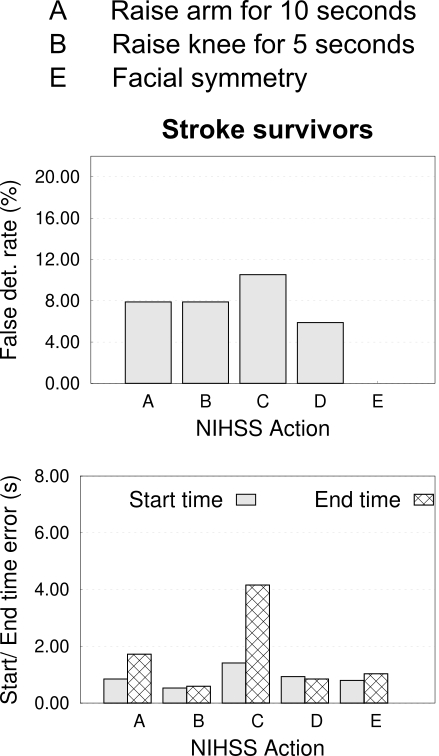
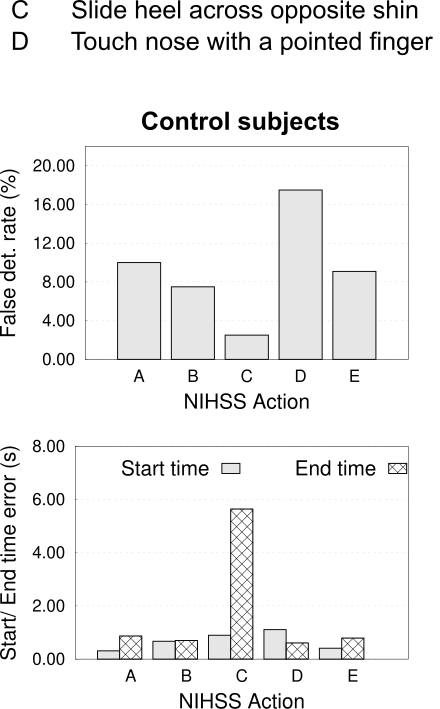
Methods: A multi-sensor prototype, including a wide-angle RGB-D camera, a high-resolution camera, and a microphone, was developed to detect and estimate the durations of different NIHSS test activities. In this study, we target 5 NIHSS activities: A. Raise arm for 10 seconds, B. Raise knee for 5 seconds, C. Slide heel across opposite shin, D. Touch nose with a pointed finger, and E. Facial symmetry. Our approach estimates the coordinates of postural and facial landmarks in camera images, creating a feature vector for each NIHSS activity to enable action identification. However, distinguishing specific actions is challenging as some resemble typical seated behaviors (e.g., pointing at a picture vs. raising an arm, or scratching the face vs. touching the nose). To resolve this ambiguity, we use microphone inputs with a customized speech recognition algorithm to temporally align commands with specific actions. Subjects were bought inside a routine laboratory space, where the prototype is mounted above the ground (see figure). Subjects performed 5 NIHSS activities, with action durations measured manually. The sensor simultaneously ran the algorithms to detect and estimate the durations automatically.
Results: Ten stroke survivors (mean age: 62.4 years, standard deviation or SD: 11.8 years) and ten control subjects (mean age: 31.6 years, SD: 17.7 years) were evaluated. False detection rates for patients were 7.9%, 7.9%, 10.5%, 5.9%, and 0.0% for NIHSS activities A to E (see figure). For control subjects, false detection rates were 10.0%, 7.5%, 2.5%, 17.5%, and 9.1%. Mean start and end time errors across activities were 0.90 and 1.67 seconds for patients, and 0.68 and 1.72 seconds for controls.
Conclusion: In conclusion, the prototype demonstrated sensitivity in identifying and estimating NIHSS activity durations for acute stroke assessment. This technology holds the potential for personalized stroke assessments across various settings, including home, ambulance, emergency room, and hospital, enabling timely intervention to address treatment needs and outcome assessments.
Saadat, Moh
(
University of South Carolina
, Columbia , South Carolina , United States )
Titus, Ryan
(
Prisma Health USC Med Group
, Columbia , South Carolina , United States )
Verkuilen, Haley
(
Prisma Health USC Med Group
, Columbia , South Carolina , United States )
Fleming, Phil
(
Prisma Health USC Med Group
, Columbia , South Carolina , United States )
Sur, Sanjib
(
University of South Carolina
, Columbia , South Carolina , United States )
Sen, Souvik
(
Prisma Health USC Med Group
, Columbia , South Carolina , United States )
Author Disclosures:
Moh Saadat:DO NOT have relevant financial relationships
| Ryan Titus:DO NOT have relevant financial relationships
| Haley VerKuilen:DO NOT have relevant financial relationships
| Phil Fleming:DO NOT have relevant financial relationships
| Sanjib Sur:DO NOT have relevant financial relationships
| Souvik Sen:DO NOT have relevant financial relationships