Cerebral Amyloid Angiopathy Prevalence and Associated Risk of Subsequent Ischemic and Hemorrhagic Stroke and Mortality in a Nationally Representative Sample
Abstract Body: Introduction: Cerebral amyloid angiopathy (CAA) is a significant cause of cerebrovascular disease and cognitive decline in elderly patients. There are limited population-based data regarding the prevalence of CAA and associated risks of mortality and incident cerebrovascular events.
Methods: We performed a retrospective cohort study using inpatient and outpatient claims from 2008 to 2018 from a nationally representative 5% sample of Medicare beneficiaries. CAA and ischemic and hemorrhagic stroke were identified using previously validated ICD-10 codes. Mortality data was obtained from Medicare beneficiary files. We calculated prevalence of CAA during 2016-2018, and used Cox regression to examine the association of CAA with subsequent death and incident stroke after adjustment for demographics, vascular risk factors, and Charlson comorbidities.
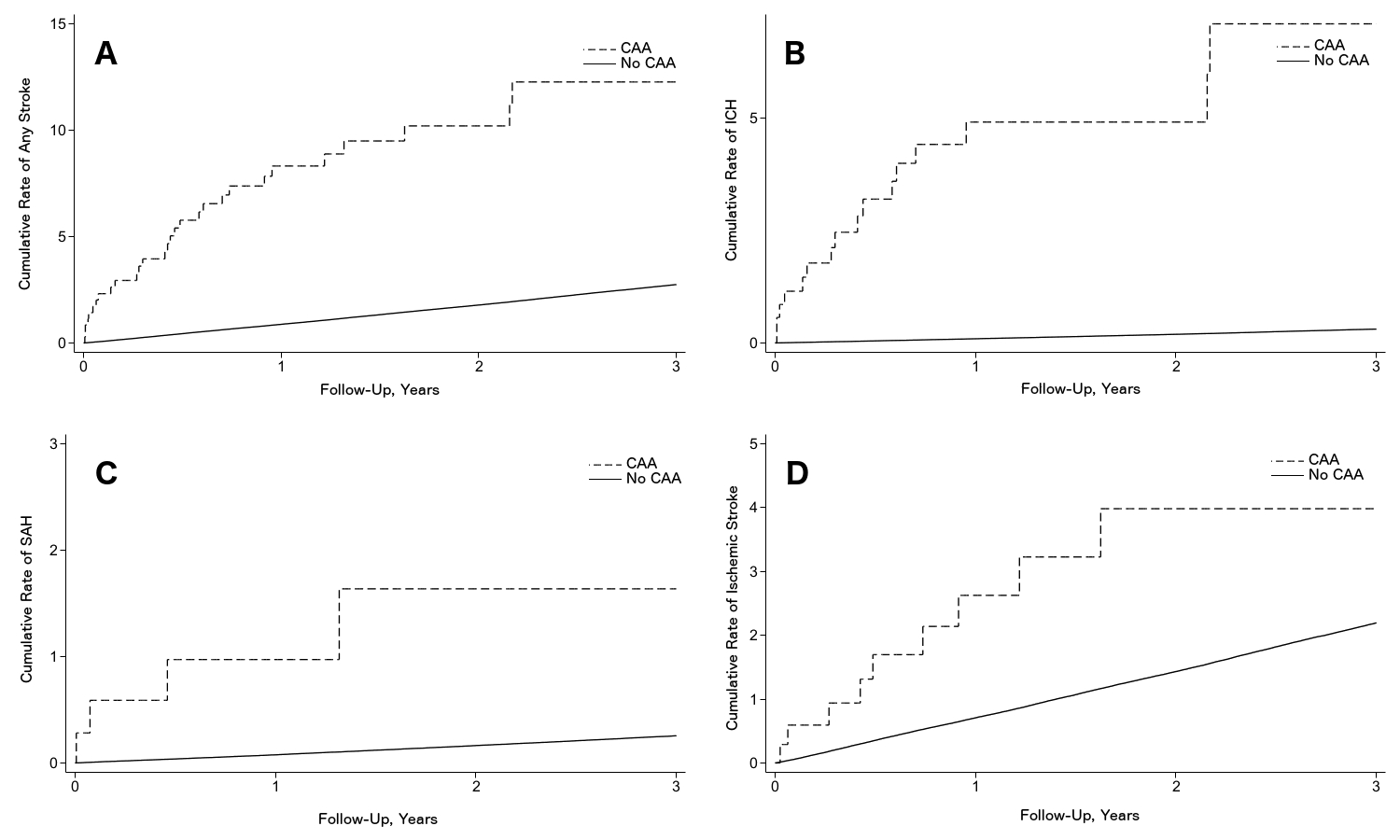
Results: Among 1,487,851 Medicare beneficiaries in our sample, 913 (0.06%) had a diagnosis of CAA during 2016-2018. In multivariable Cox regression analysis, there was no association between CAA and subsequent mortality (adjusted hazard ratio [aHR], 1.2; 95% CI, 0.7-1.9). Among 1,455,257 patients without prevalent stroke, including 355 of the CAA patients, there was a significant association between CAA and subsequent increased risk of any stroke (aHR, 6.3; 95% CI, 4.4-9.1), ischemic stroke (aHR, 2.5; 95% CI, 1.3-4.7), intracerebral hemorrhage (aHR, 32.1; 95% CI, 19.6-52.4), and subarachnoid hemorrhage (aHR, 9.5; 95% CI, 3.6-25.4) [Figure 1].
Conclusions: In a nationally representative cohort of Medicare beneficiaries, the prevalence of clinically diagnosed CAA was approximately 6 per 10,000. CAA was not associated with an increased risk of mortality but was associated with an increased risk of incident stroke, both hemorrhagic and ischemic.
Bruce, Samuel
(
Weill Cornell Medicine
, New York , New York , United States )
Zhang, Cenai
(
Weill Cornell Medicine
, New York , New York , United States )
Liberman, Ava
(
Weill Cornell Medicine
, New York , New York , United States )
Merkler, Alexander
(
Weill Cornell Medicine
, New York , New York , United States )
Navi, Babak
(
Weill Cornell Medicine
, New York , New York , United States )
Chiang, Gloria
(
Weill Cornell Medicine
, New York , New York , United States )
Iadecola, Costantino
(
Weill Cornell Medicine
, New York , New York , United States )
Kamel, Hooman
(
Weill Cornell Medicine
, New York , New York , United States )
Murthy, Santosh
(
Weill Cornell Medicine
, New York , New York , United States )
Author Disclosures:
Samuel Bruce:DO NOT have relevant financial relationships
| Cenai Zhang:DO NOT have relevant financial relationships
| Ava Liberman:No Answer
| Alexander Merkler:No Answer
| Babak Navi:DO NOT have relevant financial relationships
| Gloria Chiang:DO have relevant financial relationships
;
Consultant:Life Molecular Imaging:Active (exists now)
; Speaker:Peerview CME:Past (completed)
; Speaker:Efficient CME:Past (completed)
; Consultant:Minoryx:Active (exists now)
| Costantino Iadecola:DO NOT have relevant financial relationships
| Hooman Kamel:DO have relevant financial relationships
;
Other (please indicate in the box next to the company name):Financial disclosures for Hooman Kamel: a PI role in the ARCADIA trial, which received in-kind study drug from the BMS-Pfizer Alliance for Eliquis and ancillary study support from Roche Diagnostics; a Deputy Editor role for JAMA Neurology; clinical trial steering/executive committee roles for the STROKE-AF (Medtronic), LIBREXIA-AF (Janssen), and LAAOS-4 (Boston Scientific) trials; consulting or endpoint adjudication committee roles for AbbVie, AstraZeneca, Boehringer Ingelheim, and Novo Nordisk; and household ownership interests in TETMedical, Spectrum Plastics Group, and Ascential Technologies.:Active (exists now)
| Santosh Murthy:DO NOT have relevant financial relationships