Racial, Ethnic and Rural Disparities in Access to Acute Stroke Capabilities Persist even with Telestroke
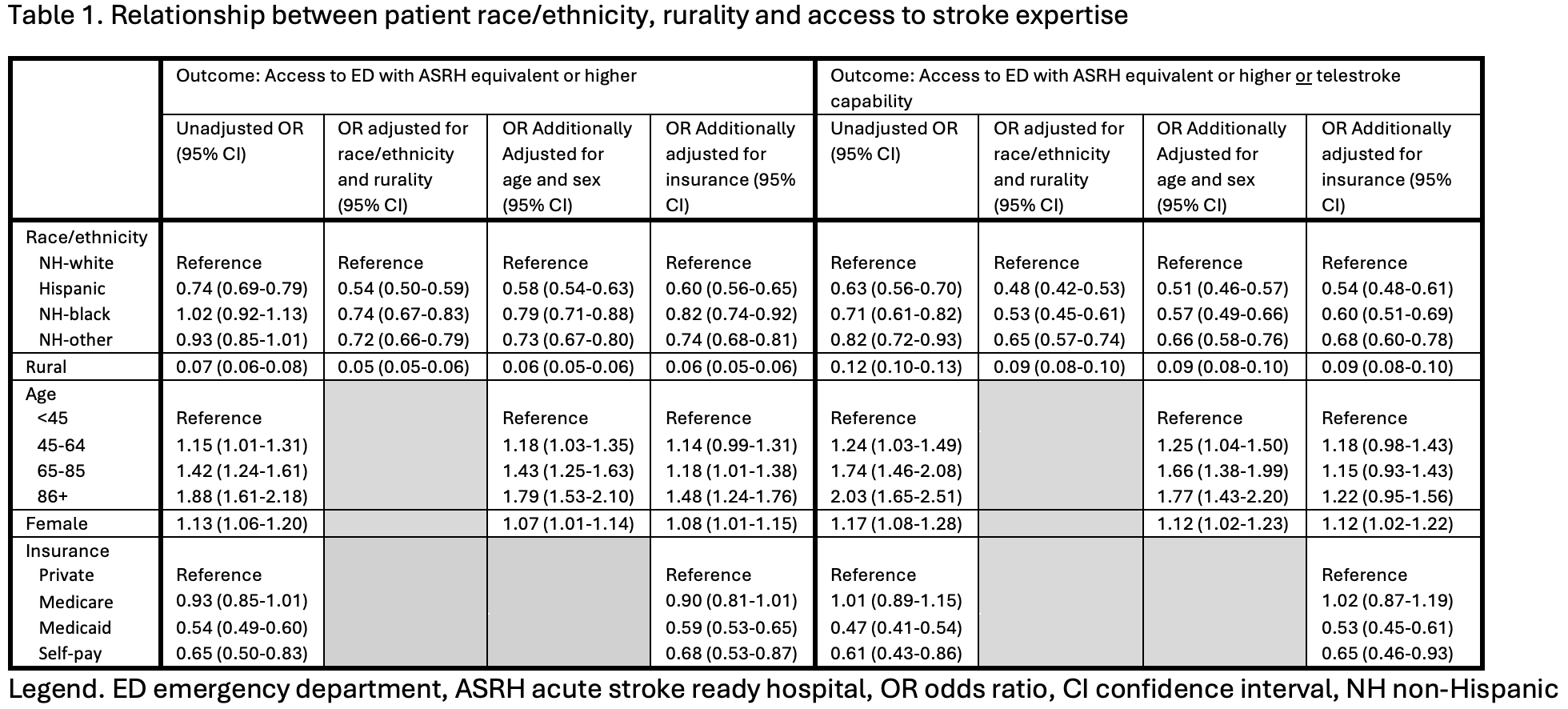
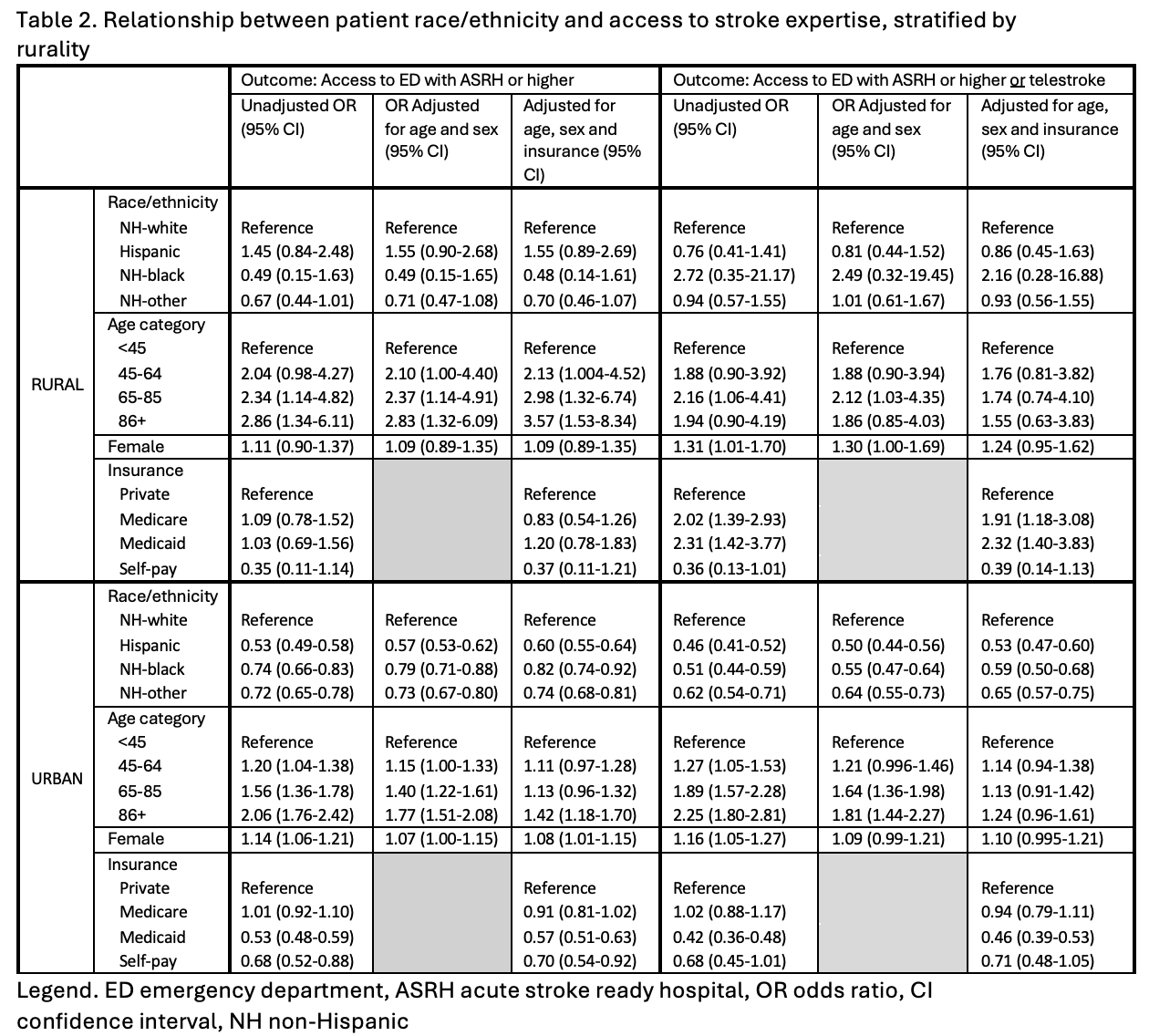
Abstract Body: Background: Telestroke may mitigate racial/ethnic and rural disparities in access to acute stroke expertise. Objective: to examine the relationship between patient race/ethnicity and presentation to an emergency department (ED) with acute stroke capabilities, including telestroke, and whether this varied by rurality. Methods: Data maintained by the California Department of Health Care Access and Information identified all statewide acute stroke encounters in 2021. ED capabilities were from the 2021 National ED Inventory-USA database (e.g., telestroke capability). ED acute stroke capabilities were defined as any stroke center status (including acute stroke ready hospital or equivalent) or telestroke capability. Logistic regression models examined the association between patient race/ethnicity, rurality and presentation to an ED with acute stroke capabilities, accounting for age, sex, and expected payer, overall and stratified by rurality. Our first outcome of interest was presentation to an ED with any stroke center status. Then, to examine whether access improved with inclusion of telestroke, the outcome included presentation to an ED with any stroke center status or telestroke capability. Results: In 2021, 264 of 325 California EDs (81%) had acute stroke capabilities, 52% with telestroke (with or without stroke center status). Of 63,252 encounters, 2,050 (3%) presented to an ED without capabilities. Overall, Hispanic, non-Hispanic patients of non-White race and rural patients had lower odds of access to acute stroke capabilities (Table 1). Odds of access did not improve with inclusion of EDs with telestroke (Table 1). When stratified by rurality, there were no differences in access by race/ethnicity for rural patients, but urban Hispanic, urban non-Hispanic Black and urban non-Hispanic patients of other race had lower odds of access relative to urban non-Hispanic White patients (Table 2). Conclusions: Most California EDs have acute stroke capabilities, with few patients presenting to non-capable centers. Overall, rural patients had lower odds of presenting to an ED with capabilities. Racial/ethnic disparities in access were distinct between urban and rural settings, with no racial/ethnic disparity among rural patients but lower odds of access for Hispanic and non-white urban patients. The inclusion of ED telestroke capability in the definition of acute stroke capabilities did not mitigate disparities in access.
Zachrison, Kori
(
Massachusetts General Hospital
, Boston , Massachusetts , United States )
Hsia, Renee
(
UCSF
, San Francisco , California , United States )
Boggs, Krislyn
(
Massachusetts General Hospital
, Boston , Massachusetts , United States )
Gao, Jingya
(
Massachusetts General Hospital
, Boston , Massachusetts , United States )
Messac, Luke
(
Brigham and Women's Hospital
, Boston , Massachusetts , United States )
Schwamm, Lee
(
Yale School of Medicine
, New Haven , Connecticut , United States )
Reeves, Mathew
(
MICHIGAN STATE UNIVERSITY
, East Lansing , Michigan , United States )
Fung, Vicki
(
Massachusetts General Hospital
, Boston , Massachusetts , United States )
Samuels-kalow, Margaret
(
Massachusetts General Hospital
, Boston , Massachusetts , United States )
Camargo, Carlos
(
MASSACHUSETTS GENERAL HOSP
, Boston , Massachusetts , United States )
Author Disclosures:
Kori Zachrison:DO NOT have relevant financial relationships
| Carlos Camargo:DO NOT have relevant financial relationships
| Renee Hsia:No Answer
| Krislyn Boggs:DO NOT have relevant financial relationships
| Jingya Gao:DO NOT have relevant financial relationships
| Luke Messac:No Answer
| Lee Schwamm:DO have relevant financial relationships
;
Consultant:genentech:Active (exists now)
; Advisor:Penumbra:Past (completed)
; Consultant:medtronic:Active (exists now)
| Mathew Reeves:DO NOT have relevant financial relationships
| Vicki Fung:DO have relevant financial relationships
;
Research Funding (PI or named investigator):NIH:Active (exists now)
; Consultant:Brandeis University:Active (exists now)
; Employee:Mass General Brigham:Active (exists now)
; Research Funding (PI or named investigator):AHRQ:Active (exists now)
| Margaret Samuels-Kalow:DO NOT have relevant financial relationships