Predictors of Certified Stroke Center Presence in the Northeastern United States
Abstract Body: Introduction: Timely intervention is essential for reducing stroke mortality, yet the distribution of AHA-certified stroke centers (SCs) is not always in line with community needs, particularly in areas with high stroke prevalence. This study examines the relationship between the presence of certified stroke centers and county-level characteristics such as demographics, stroke prevalence and mortality, risk factors, and urbanization in the northeastern United States.
Methods: Publicly available data from the U.S. Census Bureau and CDC Interactive Atlas of Heart Disease and Stroke were analyzed using a generalized linear model to examine the relationship between SC distribution and county demographics, stroke prevalence and mortality, and prevalence of stroke risk factors. Northeastern states were identified as Connecticut, Maine, Massachusetts, New Hampshire, New Jersey.
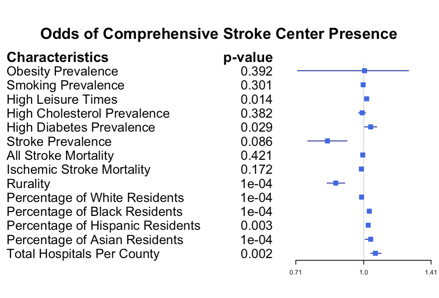
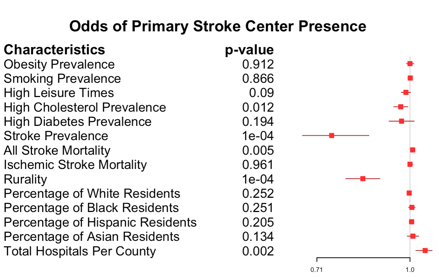
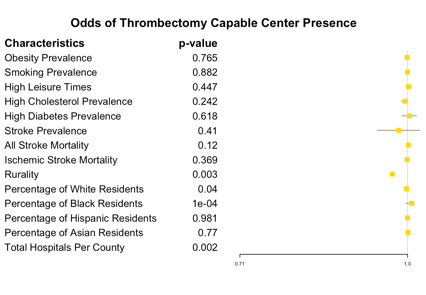
Results: Comprehensive (CSC) (adjusted odds ratio, 0.87 [95% CI, 0.83–0.91]; P<0.001), Primary (PSC) (adjusted odds ratio, 0.84 [95% CI, 0.79–0.89]; P<0.001), and Thrombectomy-Capable (TSC) (adjusted odds ratio, 0.97 [95% CI, 0.95–0.99]; P=0.003) center presence demonstrated a negative relationship with rurality. Lower overall SC density was observed in counties with high prevalence of hypercholesterolemia (adjusted odds ratio, 0.96 [95% CI, 0.93–0.99]; P=0.003). The absence of a CSC or PSC in a county was associated with a mean household income decrease of over $9,000 (P=0.005; P<0.001, respectively). Additionally, higher prevalence of stroke was associated with lower odds of PSC presence (adjusted odds ratio, 0.78 [95% CI, 0.67–0.90]; P<0.001).
Conclusion: This study reveals significant disparities in certified stroke center distribution in the northeastern U.S. While these centers reduce stroke mortality, their distribution does not uniformly reflect community needs. Of particular note was the negative association between stroke prevalence and the presence of PSCs, as PSCs often serve as the care access point for stroke patients in a hub-and-spoke system. These data point to a gap in access to specialized stroke care where it is most needed. Addressing the gap requires policymakers to consider both geographic and social factors, potentially expanding stroke centers in underserved regions to improve outcomes. Future research should focus on strategies to reduce these inequities and enhance access to stroke care.
Teshome, Abigail
(
The Warren Alpert Medical School of Brown University
, Providence , Rhode Island , United States )
Taman, Mazen
(
The Warren Alpert Medical School of Brown University
, Providence , Rhode Island , United States )
Perelstein, Elizabeth
(
The Warren Alpert Medical School of Brown University
, Providence , Rhode Island , United States )
Proulx, Jeffrey
(
Brown School of Public Health
, Providence , Rhode Island , United States )
Feler, Joshua
(
The Warren Alpert Medical School of Brown University
, Providence , Rhode Island , United States )
Author Disclosures:
Abigail Teshome:DO NOT have relevant financial relationships
| Mazen Taman:DO NOT have relevant financial relationships
| Elizabeth Perelstein:DO NOT have relevant financial relationships
| Jeffrey Proulx:No Answer
| Joshua Feler:DO NOT have relevant financial relationships