Flow diversion treatments for unruptured intracranial aneurysms: real-world perioperative outcomes, hospital readmissions, and impact of comorbid anxiety and mood disorders
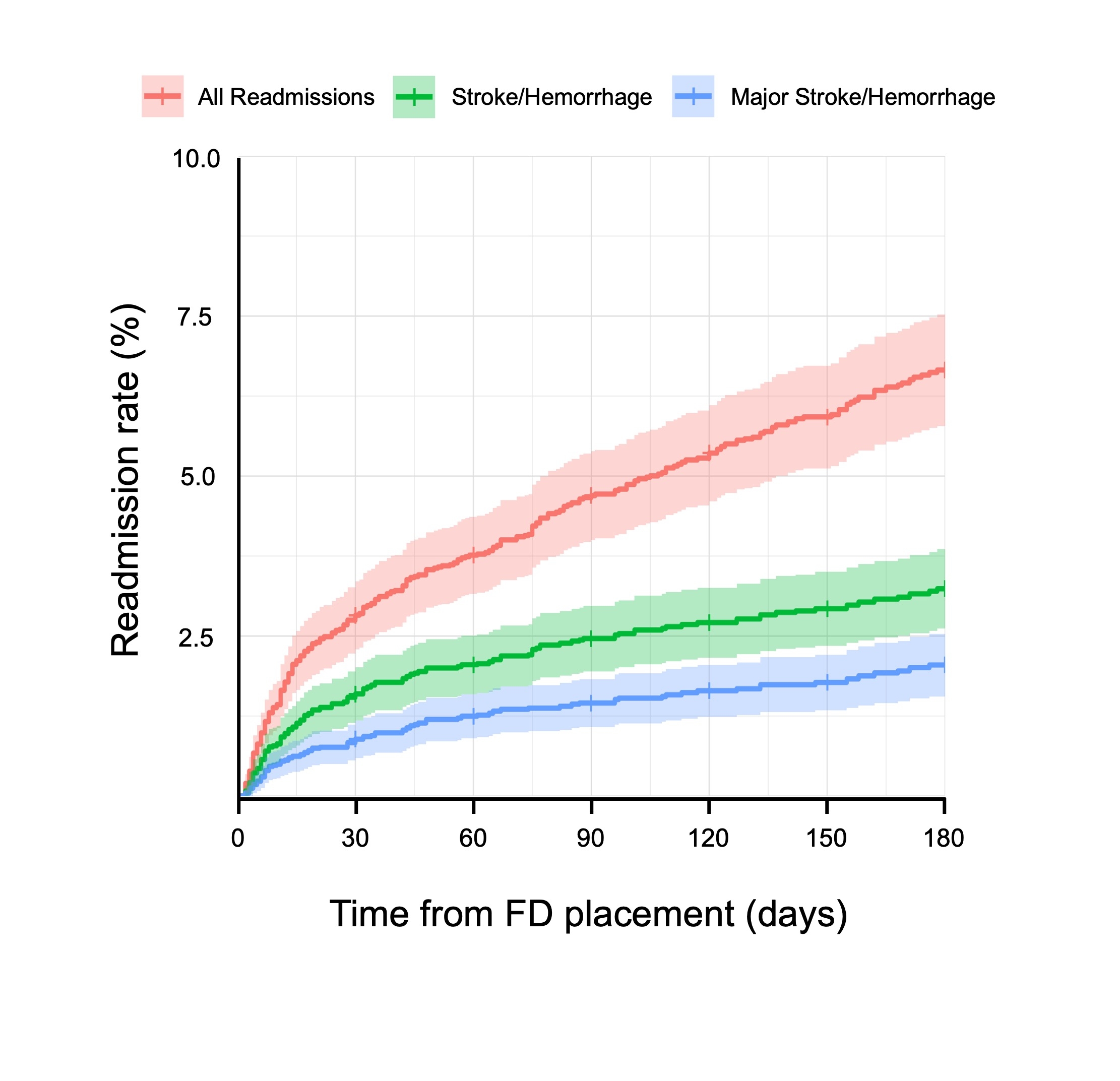
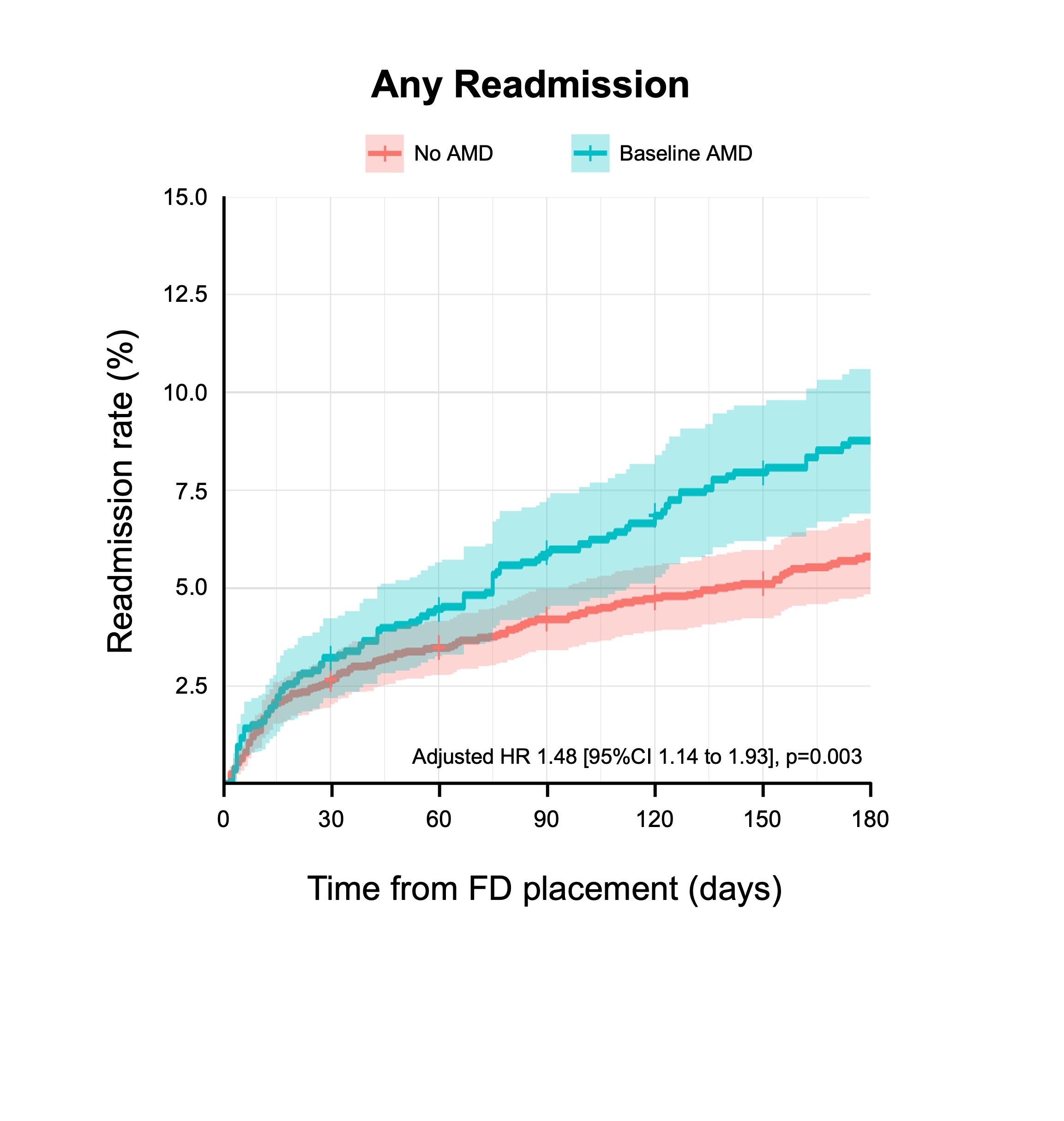
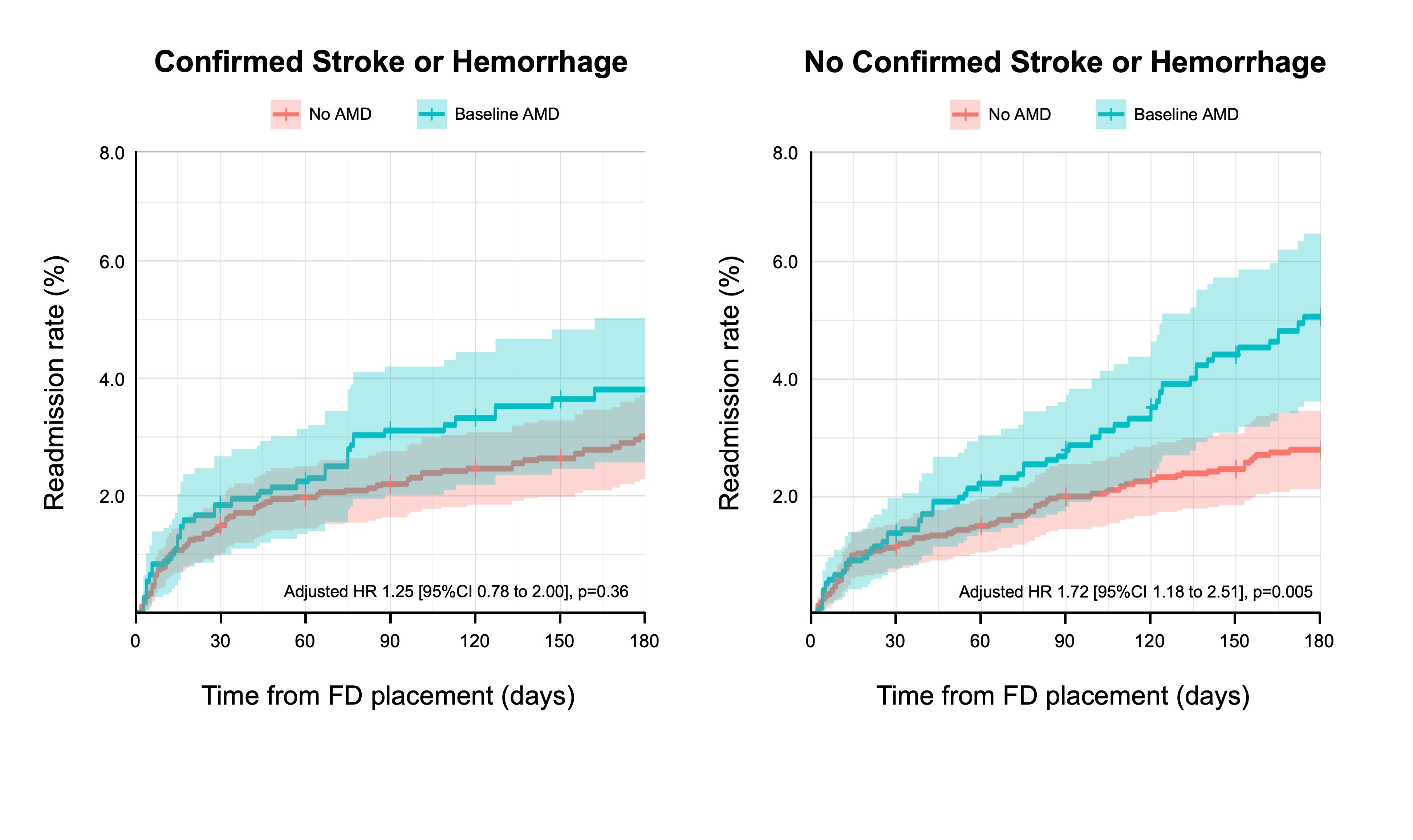
Abstract Body: Introduction: Flow diversion (FD) is a minimally invasive treatment for unruptured intracranial aneurysms (UIA) and is often preferred over open cerebrovascular surgery; however, FD patients are at risk of post-procedural stroke and hemorrhage. Furthermore, UIA patients often have comorbid anxiety and mood disorders (AMD); whether these patients are at increased risk of adverse outcomes following FD is unclear. Methods: This was a retrospective analysis of the 2020-21 National Readmissions Database (NRD) in the United States. Patients who underwent elective FD placement were identified. Initial hospitalization outcomes were assessed. Patients who had an uncomplicated FD placement were followed for the calendar year for non-elective hospital readmissions. Risks of readmission for patients with and without baseline AMD were compared using Cox regression models adjusting for major confounders. Results: 9,523 elective FD patients were identified, of whom 243 (2.6%) and 314 (3.3%) suffered perioperative stroke and intracranial hemorrhage (ICH), respectively, and 2,800 (29.4%) had baseline AMD. Six-month readmission rate for any reason, stroke or hemorrhage, and major stroke or hemorrhage (that led to patient morbidity or mortality) were 6.9%, 3.9%, and 1.8%, respectively (Figure 1). Patients with baseline AMD had a significantly higher risk of overall hospital readmissions than those without (adjusted hazards ratio 1.48 [95%CI 1.14 to 1.93], p=0.003; Figure 2). Further analyses revealed that patients with baseline AMD did not have a higher risk of any stroke or hemorrhage confirmed during readmissions (HR 1.25 [95%CI 0.78-2.00], p=0.36; Figure 3), but they did have a significantly higher risk of readmissions without confirmed stroke or hemorrhage (HR 1.72 [95%CI 1.18 to 2.51], p=0.005; Figure 3). Among readmitted AMD patients without confirmed stroke or hemorrhage, 15.4% suffered short-term morbidity, which incurred a median cost of $11,725 USD per patient. Conclusions: In routine United States clinical practice, the perioperative risks of stroke and ICH for FD patients were 2.6% and 3.3% respectively, and the risk major stroke or hemorrhage within 6 months after hospital discharge was 1.8%. Baseline AMD was associated with a significantly increased risk of hospital readmissions without confirmed stroke or hemorrhage, highlighting the need for a better understanding of how comorbid AMD may impact patient outcomes following FD.
Chen, Huanwen
(
National Institutes of Health
, Bethesda , Maryland , United States )
Khunte, Mihir
(
Brown University
, Providence , Rhode Island , United States )
Njonkou Tchoquessi, Rosy Linda
(
University of Maryland Medical Center
, Baltimore , Maryland , United States )
Miller, Tim
(
University of Maryland Medical Center
, Baltimore , Maryland , United States )
Cherian, Jacob
(
University of Maryland Medical Center
, Baltimore , Maryland , United States )
Majmundar, Shyam
(
University of Maryland Medical Center
, Baltimore , Maryland , United States )
Colasurdo, Marco
(
Oregon Health & Science University
, Portland , Oregon , United States )
Malhotra, Ajay
(
Yale University
, New Canaan , Connecticut , United States )
Gandhi, Dheeraj
(
University of Maryland Medical Center
, Baltimore , Maryland , United States )
Author Disclosures:
Huanwen Chen:DO NOT have relevant financial relationships
| Mihir Khunte:DO NOT have relevant financial relationships
| Rosy Linda Njonkou Tchoquessi:DO NOT have relevant financial relationships
| tim miller:DO NOT have relevant financial relationships
| Jacob Cherian:No Answer
| Shyam Majmundar:DO NOT have relevant financial relationships
| Marco Colasurdo:DO NOT have relevant financial relationships
| Ajay Malhotra:DO NOT have relevant financial relationships
| Dheeraj Gandhi:DO have relevant financial relationships
;
Research Funding (PI or named investigator):microvention:Active (exists now)
; Research Funding (PI or named investigator):Focused Ultrasound Foundation:Active (exists now)
; Consultant:Navigantis:Active (exists now)
; Research Funding (PI or named investigator):University of Marland:Active (exists now)
; Research Funding (PI or named investigator):NIH:Active (exists now)