Both Infarct and Non-infarcted Brain Regions Drive Acute Deep Learning Based MRI Prediction of Stroke Outcome
Abstract Body: Purpose: Predicting long-term outcomes from early acute ischemic stroke (AIS) information is crucial for prognostication, resource management, and clinical trials. Current methods predominantly depend on infarct-related features, such as size and location, for outcome predictions, and demonstrate limited correlation with outcomes. This study examines how deep learning leverages different brain regions, including non-infarct areas, to improve the accuracy of 90-day outcome predictions in AIS patients.
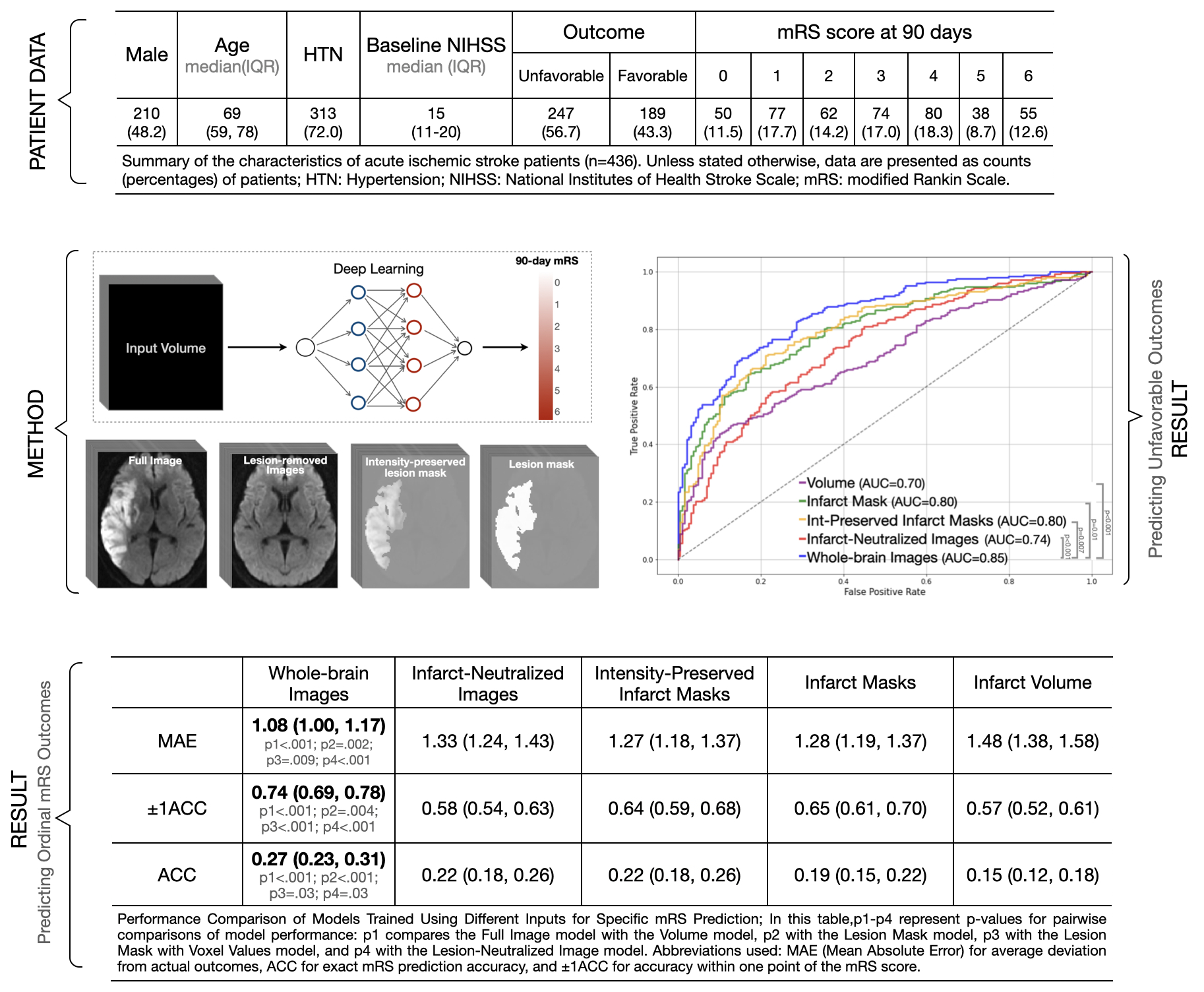
Materials and Methods: We developed and validated deep learning (DL) models on a cohort of 436 AIS patients, using MRI diffusion-weighted imaging scans from 1-7 days post-stroke and 90-day modified Rankin Scale (mRS) follow-up data. These models were trained on various inputs— infarct volumes, whole-brain images, infarct masks, intensity-preserved infarct masks, and images in which the infarct region is removed, which we call infarct-neutralized images, and which enable an assessment of overall brain health. Model performance was assessed based on the accuracy of predicting the specific mRS score, accuracy within ±1 mRS category, mean absolute error (MAE), and the ability to predict unfavorable outcomes (mRS > 2) using receiver operator curve (ROC) metrics.
Results: The infarct volume model had the highest (worst) MAE of 1.48 points (95% CI: 1.38-1.58, p < 0.001), while the whole-brain model achieved the lowest (best) MAE of 1.08 points (95% CI: 1.00-1.17). Models with intermediate imaging information—such as infarct masks (MAE 1.28, 95% CI: 1.19-1.37, p = .002), intensity-preserved infarct masks (MAE 1.27, 95% CI: 1.18-1.37, p = .009), and infarct-neutralized images (MAE 1.33, 95% CI: 1.24-1.43, p < .001)—improved upon the volume-only predictions. For predicting unfavorable outcomes, the infarct volume model had the lowest performance (AUC 0.70, 95% CI: 0.65-0.75; p < .001), while the whole-brain model achieved the highest AUC of 0.85 (95% CI: 0.82-0.89), outperforming the infarct mask (AUC 0.80, 95% CI: 0.76-0.84; p = .01), intensity-preserved infarct mask (AUC 0.80, 95% CI: 0.76-0.84; p = .007), and infarct-neutralized images (AUC 0.74, 95% CI: 0.69-0.79; p < .001)
Conclusions: The best predictive performance was achieved using voxel values from the entire brain, showing that both infarcted and non-infarcted regions contribute significantly to accuracy. Non-infarcted areas may reflect overall brain health and resilience, informing potential outcomes.
Liu, Yongkai
(
Stanford University
, Stanford , California , United States )
Van Voorst, Henk
(
Stanford University
, Stanford , California , United States )
Jiang, Bin
(
Stanford University
, Stanford , California , United States )
Yu, Yannan
(
Stanford University
, Stanford , California , United States )
Zaharchuk, Greg
(
Stanford University
, Stanford , California , United States )
Author Disclosures:
Yongkai Liu:DO NOT have relevant financial relationships
| Henk van Voorst:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Dutch Scientific Council (NWO):Active (exists now)
; Research Funding (PI or named investigator):Dutch Heart Foundation:Past (completed)
; Royalties/Patent Beneficiary:Stanford School of Medicine:Active (exists now)
; Researcher:Amsterdam UMC:Past (completed)
| Bin Jiang:No Answer
| Yannan Yu:DO NOT have relevant financial relationships
| Greg Zaharchuk:DO have relevant financial relationships
;
Ownership Interest:Subtle Medical Inc.:Active (exists now)