Risks and Benefits of Lecanemab and Anticoagulants: Results from a Simulation Model
Abstract Body: Background: In CLARITY-AD, lecanemab slowed cognitive decline but increased intracranial hemorrhages (ICHs), particularly with concurrent anticoagulant use. The Alzheimer’s Association’s expert guidance is to avoid co-prescribing; however, CMS and FDA do not restrict or warn against it. We used a microsimulation model to quantify the potential benefits and harms of co-prescribing lecanemab and apixaban in people with atrial fibrillation (AF) experiencing mild cognitive impairment or early Alzheimer’s.
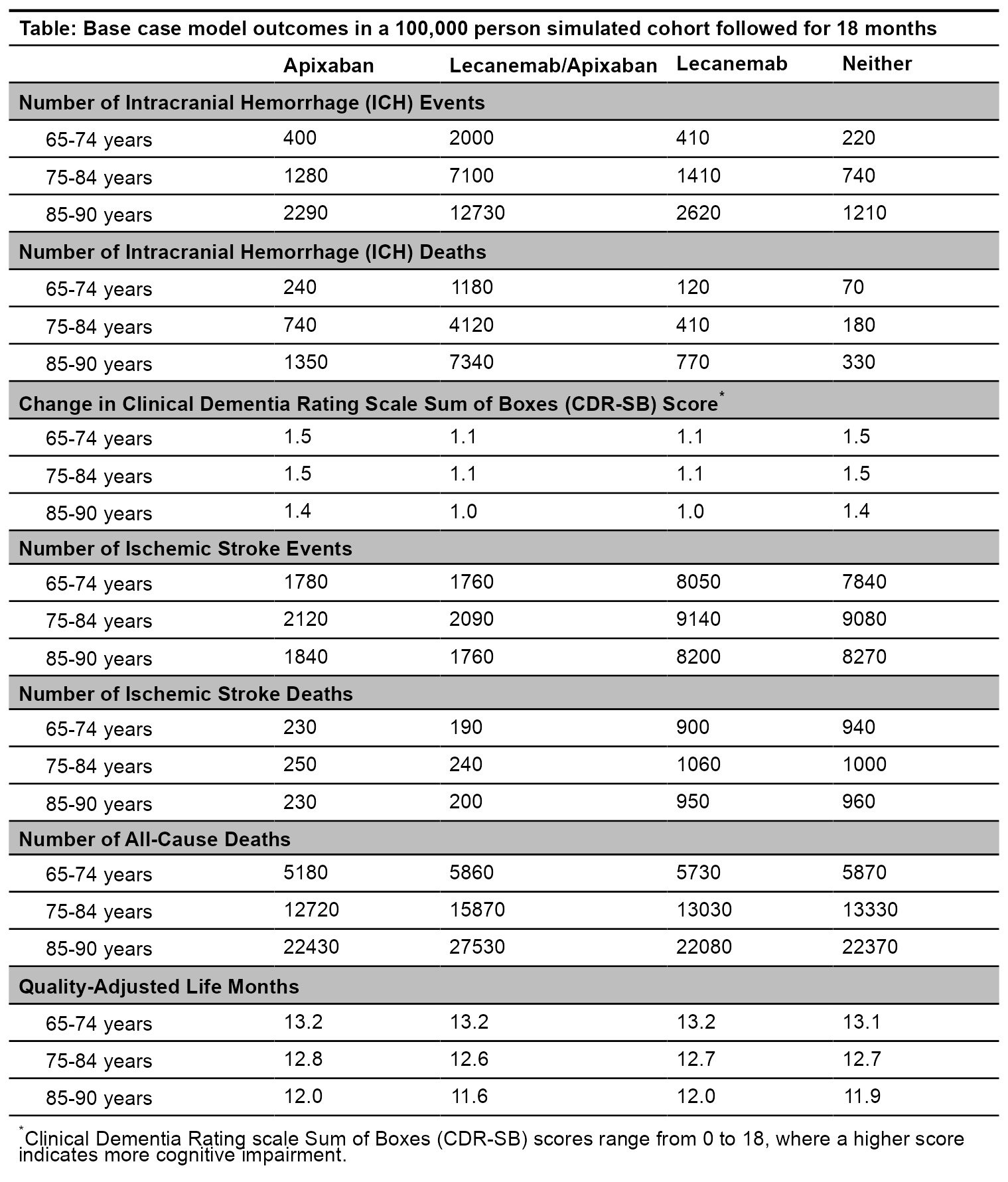
Methods: We developed a microsimulation model to estimate the health and cognition-related quality of life among persons 65-90 years with AF and cognitive impairment. We compared 4 strategies over 18 months in a cohort of 100,000 people: apixaban alone, lecanemab and apixaban, lecanemab alone, and neither. The model was populated with the Health and Retirement Study-AF cohort. Monthly model outcomes included ICH, ischemic stroke, cognitive impairment, quality-adjusted life months (QALMs), and survival. Increased ICH risk was a key input: a trial-reported 2.02-fold increase for lecanemab alone, a 1.84-fold increase for apixaban alone (anticoagulant literature), and a trial-reported 9.92-fold increase for lecanemab and anticoagulants together. We assigned quality-of-life estimates and mortality rates for people with cognitive impairment, stroke, and ICH. Background mortality rates increased with cognitive decline and following a stroke or ICH event.
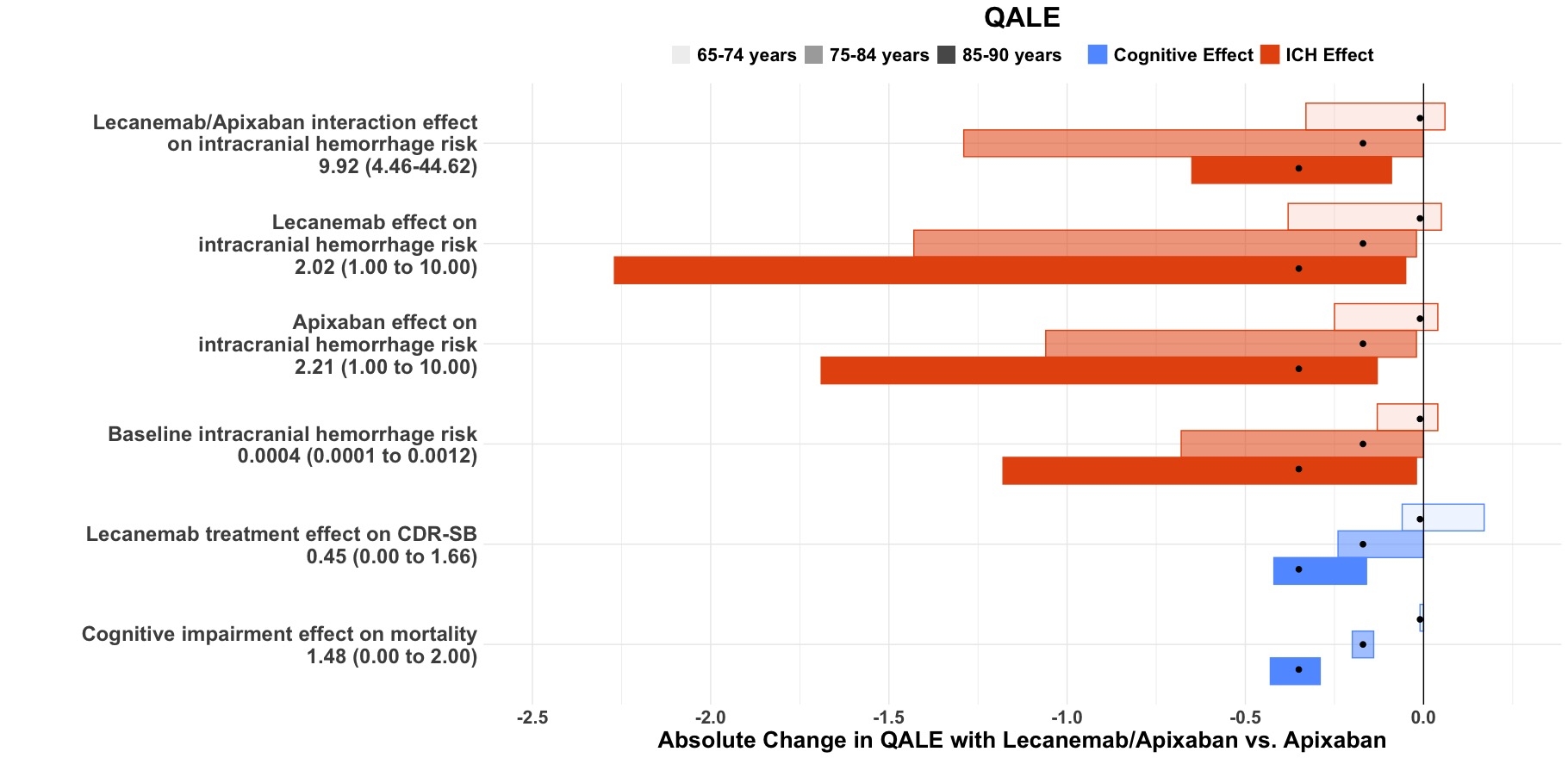
Results: For ages 65-74, apixaban alone and lecanemab added to apixaban produced a similar net benefit (13.2 QALM each, Table). Over 100,000 simulated persons aged 65-74 years, adding lecanemab to apixaban would result in greater ICH events (2000 vs. 400) and all-cause deaths (5860 vs. 5180) and slower cognitive decline (mean change in CDR-SB 1.11 vs. 1.53). One-way sensitivity analyses show that the net benefit for people aged 65-74 years is sensitive to the determinants of ICH—lecanemab/anticoagulant interaction, lecanemab effect on ICH, apixaban effect on ICH, baseline ICH risk—and lecanemab effect on CDR-SB (Figure). Apixaban alone was preferred for people 75 years and older.
Conclusion: The model-based results suggest equipoise between apixaban alone and lecanemab with apixaban for people with cognitive impairment and AF aged 65-74 years. Improving lecanemab efficacy or reducing its effect on ICH could produce a net benefit for this age group. For people 75 and older, apixaban alone would be preferred.
Shah, Sachin
(
Massachusetts General Hospital and Harvard Medical School
, Boston , Massachusetts , United States )
Dinger, Tai
(
Massachusetts General Hospital and Harvard Medical School
, Boston , Massachusetts , United States )
Blacker, Deborah
(
Massachusetts General Hospital and Harvard Medical School
, Boston , Massachusetts , United States )
Greenberg, Steven
(
Massachusetts General Hospital and Harvard Medical School
, Boston , Massachusetts , United States )
Newhouse, Joseph
(
Harvard University
, Cambridge , Massachusetts , United States )
Lykken, Jacquelyn
(
Massachusetts General Hospital and Harvard Medical School
, Boston , Massachusetts , United States )
Pandya, Ankur
(
Harvard T.H. Chan School of Public Health
, Boston , Massachusetts , United States )
Hsu, John
(
Massachusetts General Hospital and Harvard Medical School
, Boston , Massachusetts , United States )
Hyle, Emily
(
Massachusetts General Hospital and Harvard Medical School
, Boston , Massachusetts , United States )
Author Disclosures:
Sachin Shah:DO NOT have relevant financial relationships
| Tai Dinger:DO NOT have relevant financial relationships
| Deborah Blacker:No Answer
| Steven Greenberg:DO have relevant financial relationships
;
Other (please indicate in the box next to the company name):Bayer (Data Safety Committee):Active (exists now)
; Royalties/Patent Beneficiary:Up-To-Date:Active (exists now)
; Other (please indicate in the box next to the company name):Bristol Myers Squibb (Date Safety Committee):Active (exists now)
| Joseph Newhouse:DO NOT have relevant financial relationships
| Jacquelyn Lykken:DO NOT have relevant financial relationships
| Ankur Pandya:DO NOT have relevant financial relationships
| John Hsu:DO have relevant financial relationships
;
Consultant:Brandeis University:Active (exists now)
; Speaker:Invitrx:Past (completed)
; Speaker:University of South Carolina:Past (completed)
; Consultant:AltaMed:Past (completed)
; Consultant:Cambridge Health Alliance:Past (completed)
| Emily Hyle:DO NOT have relevant financial relationships