HRS8179 in Patients with Cerebral Edema after Large Hemispheric Infarction: A Multicenter, Randomized, Double-blinded, Placebo-controlled, Phase 2 Study
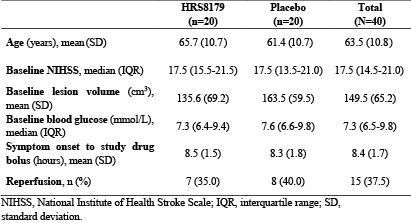
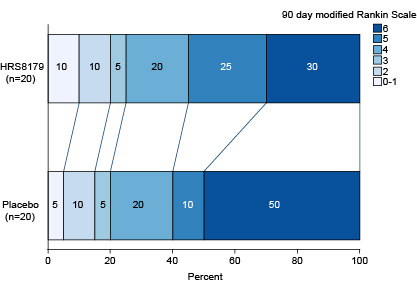
Abstract Body: Background: Large hemispheric infarction (LHI) shows a high risk of cerebral edema and neurological deterioration, even leading to death, but it still has limited treatment options. HRS8179 is a selective sulfonylurea receptor 1 inhibitor, which can block the up-regulated sodium channel after ischemic stroke and reduce cerebral edema. This study assessed HRS8179 in patients with cerebral edema after large hemispheric infarction. Methods: In this multicenter, randomized, double-blinded, placebo-controlled, phase 2 clinical trial (NCT05690711), patients who had a clinical diagnosis of LHI for <10 hours (confirmed by diffusion-weighted image or computed tomography perfusion lesion volume of 80-300 cm3) and National Institutes of Health Stroke Scale (NIHSS) ≥10 were randomized (1:1) to receive HRS8179 or placebo administered as a 0.15 mg intravenous injection followed by a 0.1 mg/h continuous intravenous infusion for 72 hours. The primary endpoint was the change in midline shift from the baseline after 72 hours of treatment. Findings: A total of 40 patients were randomized (20 in the HRS8179 group, 20 in the placebo group). Baseline characteristics were similar between groups (Table). HRS8179-treated patients had a LS mean change in midline shift relative to baseline at 72 hours of 7.92 mm, compared with 9.17 mm in placebo-treated patients (difference, -1.25 mm [95% CI, -5.50 to 3.00]). The 90-day mortality rate in the HRS8179 group and the placebo group were 30.0% (95% CI, 11.9% to 54.3%) and 50.0% (95% CI, 27.2% to 72.8%), respectively. Distribution of modified Rankin Scale scores at 90 days for both groups is shown (Figure). The increase in NIHSS ≥4 points at 72 hours occurred in 5 patients (26.3%) in the HRS8179 group and 7 patients (41.2%) in the placebo group. At 2 weeks of symptom onset, 6 patients (30.0%) in the HRS8179 group and 13 patients (65.0%) in the placebo group experienced brain herniation or death. The most common treatment-related adverse events (TRAEs) in the HRS8179 group were hypoglycemia (7 [35.0%]). The incidence of hypoglycemia with blood glucose levels <3.9 mmol/L was 30.0% and levels <3.0 mmol/L was 15.0%, which were rapidly resolved by intravenous glucose supplementation. No TRAEs led to death. Interpretation: HRS8179 showed potential efficacy in reducing the severity of cerebral edema in patients with LHI, particularly in lowering the 90-day mortality rate, even in patients without reperfusion, with an acceptable safety profile.